Marlena A Fox, Chancey Carothers, Katie K Dircksen, Kara L Birrer, Min J Choi, Satyanarayana R Mukkera
{"title":"危重症患者医源性阿片类药物戒断的患病率及危险因素","authors":"Marlena A Fox, Chancey Carothers, Katie K Dircksen, Kara L Birrer, Min J Choi, Satyanarayana R Mukkera","doi":"10.1097/CCE.0000000000000904","DOIUrl":null,"url":null,"abstract":"<p><p>Opioids are the mainstay of pain management and sedation in critically ill patients, which can lead to the development of physiologic tolerance and dependency. The prevalence of iatrogenic opioid withdrawal syndrome (IWS) is reported as 17-32% in the ICU; however, limited evidence exists for the medical ICU patient population.</p><p><strong>Objectives: </strong>To identify the and risk factors for IWS in adult patients admitted to critical care medicine services who received greater than or equal to 24 hours of continuous opioid infusion therapy.</p><p><strong>Design setting and participants: </strong>A prospective, observational study was conducted in a tertiary care hospital in adult medical ICU patients. Ninety-two patients who received greater than or equal to 24 hours of continuous opioid infusions were included in the study.</p><p><strong>Main outcomes and measurements: </strong>Patients were assessed daily after opioid infusion discontinuation using the Clinical Opiate Withdrawal Scale (COWS) and the Diagnostic and Statistical Manual of Mental Disorders (DSM-V) opioid withdrawal criteria for a maximum of 5 days. The primary outcome was the prevalence of IWS of moderate severity or greater using COWS. Secondary outcomes included the prevalence of IWS diagnosis of any severity based on COWS, the prevalence of IWS diagnosis based on a positive DSM-V score, and the identification of potential risk factors for developing IWS of any severity.</p><p><strong>Results: </strong>Four hundred forty-seven patients received greater than or equal to 24 hours of continuous opioid therapy. Of these, 385 were excluded, leaving 92 patients included in the final analysis. Except for a higher prevalence of psychiatric history in the IWS-positive group, baseline characteristics were similar. Overall, 11 patients (12%) developed IWS of moderate severity or greater, based on COWS. The IWS-positive group also had longer durations of opioid infusions, higher cumulative opioid infusion doses, higher mean daily doses, and higher infusion rates at any given time. The concomitant use of dexmedetomidine (38.3 vs 15.6%, <i>p</i> = 0.014) and benzodiazepines (63.8 vs 37.8%, <i>p</i> = 0.021) during or after the opioid infusion were significantly higher in the IWS-positive group compared with the IWS-negative group. No significant differences were found between the two groups for scheduled or as needed opioids after cessation of the opioid infusion. Continuous opioid infusions greater than or equal to 72 hours and total daily dose greater than or equal to 1,200 μg were found to be independent predictors for the development of iatrogenic opioid withdrawal via logistic regression.</p><p><strong>Conclusions and relevance: </strong>Approximately one in every eight patients receiving continuous infusion opioid for greater than 24 hours while mechanically ventilated in the medical ICU will develop IWS of moderate severity or greater; this increases to one in three patients diagnosed with DSM-V criteria or any level of IWS severity. Patients receiving opioid infusions greater than or equal to 72 hours, or a total daily fentanyl dose of greater than or equal to 1,200 μg (~ 50 μg/hr) are at a higher risk for developing IWS and should be monitored as part of clinical practice when opioid infusions are discontinued.</p>","PeriodicalId":10759,"journal":{"name":"Critical Care Explorations","volume":"5 5","pages":"e0904"},"PeriodicalIF":0.0000,"publicationDate":"2023-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/35/ce/cc9-5-e0904.PMC10158916.pdf","citationCount":"1","resultStr":"{\"title\":\"Prevalence and Risk Factors for Iatrogenic Opioid Withdrawal in Medical Critical Care Patients.\",\"authors\":\"Marlena A Fox, Chancey Carothers, Katie K Dircksen, Kara L Birrer, Min J Choi, Satyanarayana R Mukkera\",\"doi\":\"10.1097/CCE.0000000000000904\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Opioids are the mainstay of pain management and sedation in critically ill patients, which can lead to the development of physiologic tolerance and dependency. The prevalence of iatrogenic opioid withdrawal syndrome (IWS) is reported as 17-32% in the ICU; however, limited evidence exists for the medical ICU patient population.</p><p><strong>Objectives: </strong>To identify the and risk factors for IWS in adult patients admitted to critical care medicine services who received greater than or equal to 24 hours of continuous opioid infusion therapy.</p><p><strong>Design setting and participants: </strong>A prospective, observational study was conducted in a tertiary care hospital in adult medical ICU patients. Ninety-two patients who received greater than or equal to 24 hours of continuous opioid infusions were included in the study.</p><p><strong>Main outcomes and measurements: </strong>Patients were assessed daily after opioid infusion discontinuation using the Clinical Opiate Withdrawal Scale (COWS) and the Diagnostic and Statistical Manual of Mental Disorders (DSM-V) opioid withdrawal criteria for a maximum of 5 days. The primary outcome was the prevalence of IWS of moderate severity or greater using COWS. Secondary outcomes included the prevalence of IWS diagnosis of any severity based on COWS, the prevalence of IWS diagnosis based on a positive DSM-V score, and the identification of potential risk factors for developing IWS of any severity.</p><p><strong>Results: </strong>Four hundred forty-seven patients received greater than or equal to 24 hours of continuous opioid therapy. Of these, 385 were excluded, leaving 92 patients included in the final analysis. Except for a higher prevalence of psychiatric history in the IWS-positive group, baseline characteristics were similar. Overall, 11 patients (12%) developed IWS of moderate severity or greater, based on COWS. The IWS-positive group also had longer durations of opioid infusions, higher cumulative opioid infusion doses, higher mean daily doses, and higher infusion rates at any given time. The concomitant use of dexmedetomidine (38.3 vs 15.6%, <i>p</i> = 0.014) and benzodiazepines (63.8 vs 37.8%, <i>p</i> = 0.021) during or after the opioid infusion were significantly higher in the IWS-positive group compared with the IWS-negative group. No significant differences were found between the two groups for scheduled or as needed opioids after cessation of the opioid infusion. Continuous opioid infusions greater than or equal to 72 hours and total daily dose greater than or equal to 1,200 μg were found to be independent predictors for the development of iatrogenic opioid withdrawal via logistic regression.</p><p><strong>Conclusions and relevance: </strong>Approximately one in every eight patients receiving continuous infusion opioid for greater than 24 hours while mechanically ventilated in the medical ICU will develop IWS of moderate severity or greater; this increases to one in three patients diagnosed with DSM-V criteria or any level of IWS severity. Patients receiving opioid infusions greater than or equal to 72 hours, or a total daily fentanyl dose of greater than or equal to 1,200 μg (~ 50 μg/hr) are at a higher risk for developing IWS and should be monitored as part of clinical practice when opioid infusions are discontinued.</p>\",\"PeriodicalId\":10759,\"journal\":{\"name\":\"Critical Care Explorations\",\"volume\":\"5 5\",\"pages\":\"e0904\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/35/ce/cc9-5-e0904.PMC10158916.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Care Explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000000904\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000000904","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
摘要
阿片类药物是危重患者疼痛管理和镇静的主要药物,可导致生理性耐受性和依赖性的发展。据报道,在ICU中,医源性阿片戒断综合征(IWS)的患病率为17-32%;然而,针对ICU患者群体的证据有限。目的:确定接受大于或等于24小时持续阿片类药物输注治疗的重症监护医学服务成年患者IWS的危险因素。设计环境和参与者:一项前瞻性观察性研究在一家三级医院进行,对象为成人内科ICU患者。92名接受大于或等于24小时连续阿片类药物输注的患者被纳入研究。主要结局和测量方法:使用临床阿片类药物戒断量表(COWS)和精神障碍诊断与统计手册(DSM-V)阿片类药物戒断标准,每天对阿片类药物输注停止后的患者进行评估,最长5天。主要终点是使用奶牛的中度或更严重的IWS患病率。次要结局包括基于母牛的任何严重程度的IWS诊断的患病率,基于DSM-V阳性评分的IWS诊断的患病率,以及确定发生任何严重程度IWS的潜在危险因素。结果:447例患者接受了大于或等于24小时的持续阿片类药物治疗。其中,385名患者被排除在外,剩下92名患者被纳入最终分析。除了iws阳性组有较高的精神病史外,基线特征相似。总体而言,11名患者(12%)发展为中度或更严重的IWS,基于奶牛。iws阳性组阿片类药物输注持续时间更长,累计阿片类药物输注剂量更高,平均每日剂量更高,任何给定时间的输注速率更高。iws阳性组在阿片类药物输注期间和输注后同时使用右美托咪定(38.3 vs 15.6%, p = 0.014)和苯二氮卓类药物(63.8 vs 37.8%, p = 0.021)的比例明显高于iws阴性组。停止阿片类药物输注后,两组之间对预定或所需阿片类药物的使用没有显着差异。通过logistic回归分析发现,阿片类药物持续输注大于或等于72小时,每日总剂量大于或等于1200 μg是发生医源性阿片类药物戒断的独立预测因素。结论和相关性:在ICU机械通气时接受阿片类药物持续输注超过24小时的患者中,大约每8名患者中就有1名会发展为中度或更严重的IWS;这一比例增加到三分之一被诊断为DSM-V标准或任何程度的IWS严重程度的患者。接受阿片类药物输注超过或等于72小时,或每日芬太尼总剂量大于或等于1200 μg (~ 50 μg/hr)的患者发生IWS的风险较高,应在停止阿片类药物输注时作为临床实践的一部分进行监测。
Prevalence and Risk Factors for Iatrogenic Opioid Withdrawal in Medical Critical Care Patients.
Opioids are the mainstay of pain management and sedation in critically ill patients, which can lead to the development of physiologic tolerance and dependency. The prevalence of iatrogenic opioid withdrawal syndrome (IWS) is reported as 17-32% in the ICU; however, limited evidence exists for the medical ICU patient population.
Objectives: To identify the and risk factors for IWS in adult patients admitted to critical care medicine services who received greater than or equal to 24 hours of continuous opioid infusion therapy.
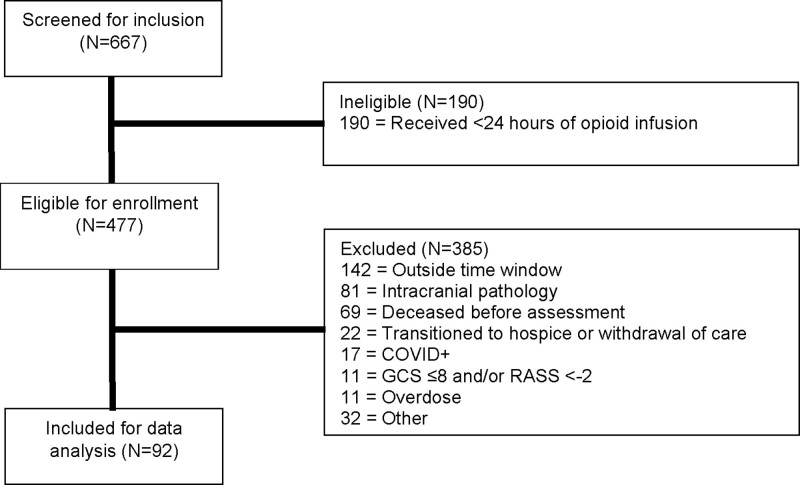
Design setting and participants: A prospective, observational study was conducted in a tertiary care hospital in adult medical ICU patients. Ninety-two patients who received greater than or equal to 24 hours of continuous opioid infusions were included in the study.
Main outcomes and measurements: Patients were assessed daily after opioid infusion discontinuation using the Clinical Opiate Withdrawal Scale (COWS) and the Diagnostic and Statistical Manual of Mental Disorders (DSM-V) opioid withdrawal criteria for a maximum of 5 days. The primary outcome was the prevalence of IWS of moderate severity or greater using COWS. Secondary outcomes included the prevalence of IWS diagnosis of any severity based on COWS, the prevalence of IWS diagnosis based on a positive DSM-V score, and the identification of potential risk factors for developing IWS of any severity.
Results: Four hundred forty-seven patients received greater than or equal to 24 hours of continuous opioid therapy. Of these, 385 were excluded, leaving 92 patients included in the final analysis. Except for a higher prevalence of psychiatric history in the IWS-positive group, baseline characteristics were similar. Overall, 11 patients (12%) developed IWS of moderate severity or greater, based on COWS. The IWS-positive group also had longer durations of opioid infusions, higher cumulative opioid infusion doses, higher mean daily doses, and higher infusion rates at any given time. The concomitant use of dexmedetomidine (38.3 vs 15.6%, p = 0.014) and benzodiazepines (63.8 vs 37.8%, p = 0.021) during or after the opioid infusion were significantly higher in the IWS-positive group compared with the IWS-negative group. No significant differences were found between the two groups for scheduled or as needed opioids after cessation of the opioid infusion. Continuous opioid infusions greater than or equal to 72 hours and total daily dose greater than or equal to 1,200 μg were found to be independent predictors for the development of iatrogenic opioid withdrawal via logistic regression.
Conclusions and relevance: Approximately one in every eight patients receiving continuous infusion opioid for greater than 24 hours while mechanically ventilated in the medical ICU will develop IWS of moderate severity or greater; this increases to one in three patients diagnosed with DSM-V criteria or any level of IWS severity. Patients receiving opioid infusions greater than or equal to 72 hours, or a total daily fentanyl dose of greater than or equal to 1,200 μg (~ 50 μg/hr) are at a higher risk for developing IWS and should be monitored as part of clinical practice when opioid infusions are discontinued.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


