Sameer Zaman, Yorissa Padayachee, Moulesh Shah, Jack Samways, Alice Auton, Nicholas M Quaife, Mark Sweeney, James P Howard, Indira Tenorio, Patrik Bachtiger, Tahereh Kamalati, Punam A Pabari, Nick W F Linton, Jamil Mayet, Nicholas S Peters, Carys Barton, Graham D Cole, Carla M Plymen
{"title":"基于智能手机的心力衰竭远程监测降低射血分数:二次护理使用和成本的回顾性队列研究。","authors":"Sameer Zaman, Yorissa Padayachee, Moulesh Shah, Jack Samways, Alice Auton, Nicholas M Quaife, Mark Sweeney, James P Howard, Indira Tenorio, Patrik Bachtiger, Tahereh Kamalati, Punam A Pabari, Nick W F Linton, Jamil Mayet, Nicholas S Peters, Carys Barton, Graham D Cole, Carla M Plymen","doi":"10.2196/45611","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Despite effective therapies, the economic burden of heart failure with reduced ejection fraction (HFrEF) is driven by frequent hospitalizations. Treatment optimization and admission avoidance rely on frequent symptom reviews and monitoring of vital signs. Remote monitoring (RM) aims to prevent admissions by facilitating early intervention, but the impact of noninvasive, smartphone-based RM of vital signs on secondary health care use and costs in the months after a new diagnosis of HFrEF is unknown.</p><p><strong>Objective: </strong>The purpose of this study is to conduct a secondary care health use and health-economic evaluation for patients with HFrEF using smartphone-based noninvasive RM and compare it with matched controls receiving usual care without RM.</p><p><strong>Methods: </strong>We conducted a retrospective study of 2 cohorts of newly diagnosed HFrEF patients, matched 1:1 for demographics, socioeconomic status, comorbidities, and HFrEF severity. They are (1) the RM group, with patients using the RM platform for >3 months and (2) the control group, with patients referred before RM was available who received usual heart failure care without RM. Emergency department (ED) attendance, hospital admissions, outpatient use, and the associated costs of this secondary care activity were extracted from the Discover data set for a 3-month period after diagnosis. Platform costs were added for the RM group. Secondary health care use and costs were analyzed using Kaplan-Meier event analysis and Cox proportional hazards modeling.</p><p><strong>Results: </strong>A total of 146 patients (mean age 63 years; 42/146, 29% female) were included (73 in each group). The groups were well-matched for all baseline characteristics except hypertension (P=.03). RM was associated with a lower hazard of ED attendance (hazard ratio [HR] 0.43; P=.02) and unplanned admissions (HR 0.26; P=.02). There were no differences in elective admissions (HR 1.03, P=.96) or outpatient use (HR 1.40; P=.18) between the 2 groups. These differences were sustained by a univariate model controlling for hypertension. Over a 3-month period, secondary health care costs were approximately 4-fold lower in the RM group than the control group, despite the additional cost of RM itself (mean cost per patient GBP £465, US $581 vs GBP £1850, US $2313, respectively; P=.04).</p><p><strong>Conclusions: </strong>This retrospective cohort study shows that smartphone-based RM of vital signs is feasible for HFrEF. This type of RM was associated with an approximately 2-fold reduction in ED attendance and a 4-fold reduction in emergency admissions over just 3 months after a new diagnosis with HFrEF. Costs were significantly lower in the RM group without increasing outpatient demand. This type of RM could be adjunctive to standard care to reduce admissions, enabling other resources to help patients unable to use RM.</p>","PeriodicalId":14706,"journal":{"name":"JMIR Cardio","volume":"7 ","pages":"e45611"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10334716/pdf/","citationCount":"0","resultStr":"{\"title\":\"Smartphone-Based Remote Monitoring in Heart Failure With Reduced Ejection Fraction: Retrospective Cohort Study of Secondary Care Use and Costs.\",\"authors\":\"Sameer Zaman, Yorissa Padayachee, Moulesh Shah, Jack Samways, Alice Auton, Nicholas M Quaife, Mark Sweeney, James P Howard, Indira Tenorio, Patrik Bachtiger, Tahereh Kamalati, Punam A Pabari, Nick W F Linton, Jamil Mayet, Nicholas S Peters, Carys Barton, Graham D Cole, Carla M Plymen\",\"doi\":\"10.2196/45611\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Despite effective therapies, the economic burden of heart failure with reduced ejection fraction (HFrEF) is driven by frequent hospitalizations. Treatment optimization and admission avoidance rely on frequent symptom reviews and monitoring of vital signs. Remote monitoring (RM) aims to prevent admissions by facilitating early intervention, but the impact of noninvasive, smartphone-based RM of vital signs on secondary health care use and costs in the months after a new diagnosis of HFrEF is unknown.</p><p><strong>Objective: </strong>The purpose of this study is to conduct a secondary care health use and health-economic evaluation for patients with HFrEF using smartphone-based noninvasive RM and compare it with matched controls receiving usual care without RM.</p><p><strong>Methods: </strong>We conducted a retrospective study of 2 cohorts of newly diagnosed HFrEF patients, matched 1:1 for demographics, socioeconomic status, comorbidities, and HFrEF severity. They are (1) the RM group, with patients using the RM platform for >3 months and (2) the control group, with patients referred before RM was available who received usual heart failure care without RM. Emergency department (ED) attendance, hospital admissions, outpatient use, and the associated costs of this secondary care activity were extracted from the Discover data set for a 3-month period after diagnosis. Platform costs were added for the RM group. Secondary health care use and costs were analyzed using Kaplan-Meier event analysis and Cox proportional hazards modeling.</p><p><strong>Results: </strong>A total of 146 patients (mean age 63 years; 42/146, 29% female) were included (73 in each group). The groups were well-matched for all baseline characteristics except hypertension (P=.03). RM was associated with a lower hazard of ED attendance (hazard ratio [HR] 0.43; P=.02) and unplanned admissions (HR 0.26; P=.02). There were no differences in elective admissions (HR 1.03, P=.96) or outpatient use (HR 1.40; P=.18) between the 2 groups. These differences were sustained by a univariate model controlling for hypertension. Over a 3-month period, secondary health care costs were approximately 4-fold lower in the RM group than the control group, despite the additional cost of RM itself (mean cost per patient GBP £465, US $581 vs GBP £1850, US $2313, respectively; P=.04).</p><p><strong>Conclusions: </strong>This retrospective cohort study shows that smartphone-based RM of vital signs is feasible for HFrEF. This type of RM was associated with an approximately 2-fold reduction in ED attendance and a 4-fold reduction in emergency admissions over just 3 months after a new diagnosis with HFrEF. Costs were significantly lower in the RM group without increasing outpatient demand. This type of RM could be adjunctive to standard care to reduce admissions, enabling other resources to help patients unable to use RM.</p>\",\"PeriodicalId\":14706,\"journal\":{\"name\":\"JMIR Cardio\",\"volume\":\"7 \",\"pages\":\"e45611\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-06-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10334716/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JMIR Cardio\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2196/45611\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR Cardio","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/45611","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
Smartphone-Based Remote Monitoring in Heart Failure With Reduced Ejection Fraction: Retrospective Cohort Study of Secondary Care Use and Costs.
Background: Despite effective therapies, the economic burden of heart failure with reduced ejection fraction (HFrEF) is driven by frequent hospitalizations. Treatment optimization and admission avoidance rely on frequent symptom reviews and monitoring of vital signs. Remote monitoring (RM) aims to prevent admissions by facilitating early intervention, but the impact of noninvasive, smartphone-based RM of vital signs on secondary health care use and costs in the months after a new diagnosis of HFrEF is unknown.
Objective: The purpose of this study is to conduct a secondary care health use and health-economic evaluation for patients with HFrEF using smartphone-based noninvasive RM and compare it with matched controls receiving usual care without RM.
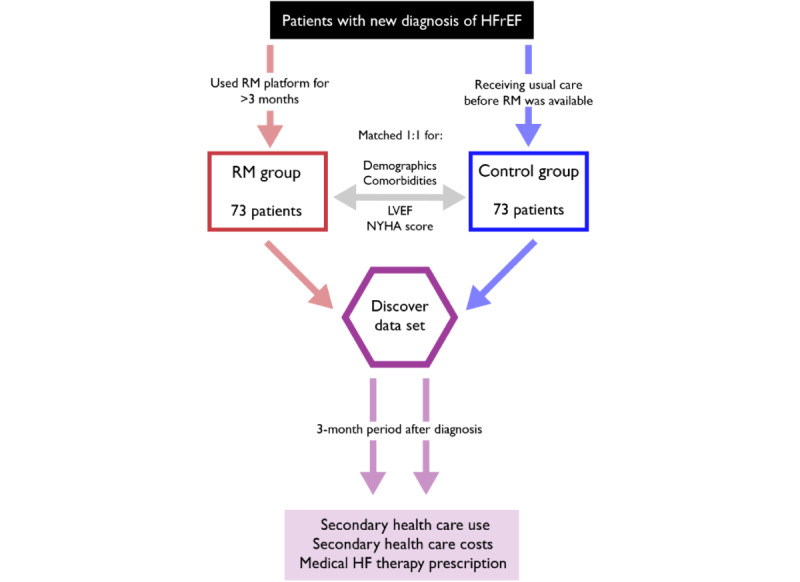
Methods: We conducted a retrospective study of 2 cohorts of newly diagnosed HFrEF patients, matched 1:1 for demographics, socioeconomic status, comorbidities, and HFrEF severity. They are (1) the RM group, with patients using the RM platform for >3 months and (2) the control group, with patients referred before RM was available who received usual heart failure care without RM. Emergency department (ED) attendance, hospital admissions, outpatient use, and the associated costs of this secondary care activity were extracted from the Discover data set for a 3-month period after diagnosis. Platform costs were added for the RM group. Secondary health care use and costs were analyzed using Kaplan-Meier event analysis and Cox proportional hazards modeling.
Results: A total of 146 patients (mean age 63 years; 42/146, 29% female) were included (73 in each group). The groups were well-matched for all baseline characteristics except hypertension (P=.03). RM was associated with a lower hazard of ED attendance (hazard ratio [HR] 0.43; P=.02) and unplanned admissions (HR 0.26; P=.02). There were no differences in elective admissions (HR 1.03, P=.96) or outpatient use (HR 1.40; P=.18) between the 2 groups. These differences were sustained by a univariate model controlling for hypertension. Over a 3-month period, secondary health care costs were approximately 4-fold lower in the RM group than the control group, despite the additional cost of RM itself (mean cost per patient GBP £465, US $581 vs GBP £1850, US $2313, respectively; P=.04).
Conclusions: This retrospective cohort study shows that smartphone-based RM of vital signs is feasible for HFrEF. This type of RM was associated with an approximately 2-fold reduction in ED attendance and a 4-fold reduction in emergency admissions over just 3 months after a new diagnosis with HFrEF. Costs were significantly lower in the RM group without increasing outpatient demand. This type of RM could be adjunctive to standard care to reduce admissions, enabling other resources to help patients unable to use RM.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


