Sujen Saravanabavan, Amneet Aulakh, Josh Douglas, Chelsea Elwood, Stephanie Erdle, Jennifer Grant, Kristopher T Kang, Natasha Kwan, Katie Lacaria, Tim T Y Lau, Colin Lee, Victor Leung, Yu-Chen Lin, Allison Mah, Anne Nguyen, Vanessa Paquette, Ashley Roberts, Melissa Watt, Julie Van Schalkwyk, Bei Yuan Zhang, Raymond Mak, Tiffany Wong
{"title":"加拿大不列颠哥伦比亚省温哥华青霉素去标签:方法、结果和未来方向的比较","authors":"Sujen Saravanabavan, Amneet Aulakh, Josh Douglas, Chelsea Elwood, Stephanie Erdle, Jennifer Grant, Kristopher T Kang, Natasha Kwan, Katie Lacaria, Tim T Y Lau, Colin Lee, Victor Leung, Yu-Chen Lin, Allison Mah, Anne Nguyen, Vanessa Paquette, Ashley Roberts, Melissa Watt, Julie Van Schalkwyk, Bei Yuan Zhang, Raymond Mak, Tiffany Wong","doi":"10.1186/s13223-023-00777-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Inaccurate penicillin allergy labels lead to inappropriate antibiotic prescriptions and harmful patient consequences. System-wide efforts are needed to remove incorrect penicillin allergy labels, but more health services research is required on how to best deliver these services.</p><p><strong>Methods: </strong>Data was extracted from five hospitals in Vancouver, British Columbia, Canada from October 2018-May 2022. The primary outcomes of this study were to outline de-labelling protocol designs, identify the roles of various healthcare professionals in de-labelling protocols and identify rates of de-labelling penicillin allergies and associated adverse events at various institutions. Our secondary outcome was to describe de-labelling rates for special populations, including pediatric, obstetric and immunocompromised subpopulations. To achieve these outcomes, participating institutions provided their de-labelling protocol designs and data on program participants. Protocols were then compared to find common themes and differences. Furthermore, adverse events were reviewed and percentages of patients de-labelled at each institution and in total were calculated.</p><p><strong>Results: </strong>Protocols demonstrated a high level of variability, including different methods of participant identification, risk-stratification and roles of providers. All protocols used oral and direct oral challenges, heavily involved pharmacists and had physician oversight. Despite the differences, of the 711 patients enrolled in all programs, 697 (98.0%) were de-labelled. There were 9 adverse events (1.3%) with oral challenges with mainly minor symptoms.</p><p><strong>Conclusions: </strong>Our data demonstrates that de-labelling programs effectively and safely remove penicillin allergy labels, including pediatric, obstetric and immunocompromised patients. Consistent with current literature, most patients with a penicillin allergy label are not allergic. De-labelling programs could benefit from increasing clinician engagement by increasing accessibility of resources to providers, including guidance for de-labelling of special populations.</p>","PeriodicalId":7702,"journal":{"name":"Allergy, Asthma, and Clinical Immunology : Official Journal of the Canadian Society of Allergy and Clinical Immunology","volume":"19 1","pages":"30"},"PeriodicalIF":0.0000,"publicationDate":"2023-04-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10114447/pdf/","citationCount":"0","resultStr":"{\"title\":\"Penicillin de-labelling in vancouver, British Columbia, Canada: comparison of approaches, outcomes and future directions.\",\"authors\":\"Sujen Saravanabavan, Amneet Aulakh, Josh Douglas, Chelsea Elwood, Stephanie Erdle, Jennifer Grant, Kristopher T Kang, Natasha Kwan, Katie Lacaria, Tim T Y Lau, Colin Lee, Victor Leung, Yu-Chen Lin, Allison Mah, Anne Nguyen, Vanessa Paquette, Ashley Roberts, Melissa Watt, Julie Van Schalkwyk, Bei Yuan Zhang, Raymond Mak, Tiffany Wong\",\"doi\":\"10.1186/s13223-023-00777-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Inaccurate penicillin allergy labels lead to inappropriate antibiotic prescriptions and harmful patient consequences. System-wide efforts are needed to remove incorrect penicillin allergy labels, but more health services research is required on how to best deliver these services.</p><p><strong>Methods: </strong>Data was extracted from five hospitals in Vancouver, British Columbia, Canada from October 2018-May 2022. The primary outcomes of this study were to outline de-labelling protocol designs, identify the roles of various healthcare professionals in de-labelling protocols and identify rates of de-labelling penicillin allergies and associated adverse events at various institutions. Our secondary outcome was to describe de-labelling rates for special populations, including pediatric, obstetric and immunocompromised subpopulations. To achieve these outcomes, participating institutions provided their de-labelling protocol designs and data on program participants. Protocols were then compared to find common themes and differences. Furthermore, adverse events were reviewed and percentages of patients de-labelled at each institution and in total were calculated.</p><p><strong>Results: </strong>Protocols demonstrated a high level of variability, including different methods of participant identification, risk-stratification and roles of providers. All protocols used oral and direct oral challenges, heavily involved pharmacists and had physician oversight. Despite the differences, of the 711 patients enrolled in all programs, 697 (98.0%) were de-labelled. There were 9 adverse events (1.3%) with oral challenges with mainly minor symptoms.</p><p><strong>Conclusions: </strong>Our data demonstrates that de-labelling programs effectively and safely remove penicillin allergy labels, including pediatric, obstetric and immunocompromised patients. Consistent with current literature, most patients with a penicillin allergy label are not allergic. De-labelling programs could benefit from increasing clinician engagement by increasing accessibility of resources to providers, including guidance for de-labelling of special populations.</p>\",\"PeriodicalId\":7702,\"journal\":{\"name\":\"Allergy, Asthma, and Clinical Immunology : Official Journal of the Canadian Society of Allergy and Clinical Immunology\",\"volume\":\"19 1\",\"pages\":\"30\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-04-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10114447/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Allergy, Asthma, and Clinical Immunology : Official Journal of the Canadian Society of Allergy and Clinical Immunology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13223-023-00777-4\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Allergy, Asthma, and Clinical Immunology : Official Journal of the Canadian Society of Allergy and Clinical Immunology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13223-023-00777-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Penicillin de-labelling in vancouver, British Columbia, Canada: comparison of approaches, outcomes and future directions.
Background: Inaccurate penicillin allergy labels lead to inappropriate antibiotic prescriptions and harmful patient consequences. System-wide efforts are needed to remove incorrect penicillin allergy labels, but more health services research is required on how to best deliver these services.
Methods: Data was extracted from five hospitals in Vancouver, British Columbia, Canada from October 2018-May 2022. The primary outcomes of this study were to outline de-labelling protocol designs, identify the roles of various healthcare professionals in de-labelling protocols and identify rates of de-labelling penicillin allergies and associated adverse events at various institutions. Our secondary outcome was to describe de-labelling rates for special populations, including pediatric, obstetric and immunocompromised subpopulations. To achieve these outcomes, participating institutions provided their de-labelling protocol designs and data on program participants. Protocols were then compared to find common themes and differences. Furthermore, adverse events were reviewed and percentages of patients de-labelled at each institution and in total were calculated.
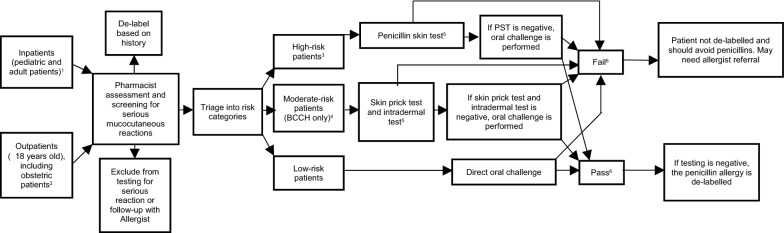
Results: Protocols demonstrated a high level of variability, including different methods of participant identification, risk-stratification and roles of providers. All protocols used oral and direct oral challenges, heavily involved pharmacists and had physician oversight. Despite the differences, of the 711 patients enrolled in all programs, 697 (98.0%) were de-labelled. There were 9 adverse events (1.3%) with oral challenges with mainly minor symptoms.
Conclusions: Our data demonstrates that de-labelling programs effectively and safely remove penicillin allergy labels, including pediatric, obstetric and immunocompromised patients. Consistent with current literature, most patients with a penicillin allergy label are not allergic. De-labelling programs could benefit from increasing clinician engagement by increasing accessibility of resources to providers, including guidance for de-labelling of special populations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


