{"title":"一个离奇的副肿瘤骨化三醇介导的高钙血症病例。","authors":"Preet Mukesh Shah, Saadia Saeed, Susana Gonzalez","doi":"10.1530/EDM-22-0371","DOIUrl":null,"url":null,"abstract":"<p><strong>Summary: </strong>A 77-year-old female patient with a history of treated breast cancer and a recently diagnosed laryngeal cancer presented with severe hypercalcaemia associated with suppressed parathyroid hormone (PTH) levels. Her initial investigations included 25-hydroxy vitamin D levels, short synacthen test, bone scan, myeloma screen and thyroid function tests which were within normality. A computerised tomography (CT) scan showed some right lung apical fibrotic changes. Her PTH-related peptide (PTHrP) was normal and sarcoidosis was also excluded. Her previous and current malignancies were thought to be unlikely behind her hypercalcaemia. Her 1,25-dihydroxy vitamin D (calcitriol) levels were found to be elevated. Her hypercalcaemia was initially managed with intravenous fluids and intermittent bisphosphonates infusions which would transiently reduce her calcium levels. Steroid treatment was initiated which improved her hypercalcaemia; however, the calcium levels rebounded on tapering the steroids down, a pre-requisite prior to a positron emission computerised tomography (PET-CT) scan to determine the source of the excess calcitriol production. This was cancelled following an emergency admission with marked hypercalcaemia and acute renal and liver injury. A contemporary CT scan showed a right apical lung mass with hepatic lesions suggestive of a disseminated lung primary. The histology obtained from a liver biopsy was compatible with metastatic small-cell lung carcinoma. Unfortunately, her clinical condition deteriorated further and she did not survive. To the best of our knowledge, this is the first report in the literature describing calcitriol-mediated hypercalcaemia due to a small-cell lung cancer.</p><p><strong>Learning points: </strong>Paraneoplastic hypercalcaemia may manifest even without overt detection of the primary cancer. The workup for paraneoplastic hypercalcaemia should be meticulous. Both bisphosphonates and steroids are useful in the initial management of calcitriol-mediated hypercalcaemia, but the definitive management is the treatment of the cause.</p>","PeriodicalId":37467,"journal":{"name":"Endocrinology, Diabetes and Metabolism Case Reports","volume":null,"pages":null},"PeriodicalIF":0.7000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/53/72/EDM22-0371.PMC10337579.pdf","citationCount":"0","resultStr":"{\"title\":\"An uncanny case of paraneoplastic calcitriol mediated hypercalcaemia.\",\"authors\":\"Preet Mukesh Shah, Saadia Saeed, Susana Gonzalez\",\"doi\":\"10.1530/EDM-22-0371\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Summary: </strong>A 77-year-old female patient with a history of treated breast cancer and a recently diagnosed laryngeal cancer presented with severe hypercalcaemia associated with suppressed parathyroid hormone (PTH) levels. Her initial investigations included 25-hydroxy vitamin D levels, short synacthen test, bone scan, myeloma screen and thyroid function tests which were within normality. A computerised tomography (CT) scan showed some right lung apical fibrotic changes. Her PTH-related peptide (PTHrP) was normal and sarcoidosis was also excluded. Her previous and current malignancies were thought to be unlikely behind her hypercalcaemia. Her 1,25-dihydroxy vitamin D (calcitriol) levels were found to be elevated. Her hypercalcaemia was initially managed with intravenous fluids and intermittent bisphosphonates infusions which would transiently reduce her calcium levels. Steroid treatment was initiated which improved her hypercalcaemia; however, the calcium levels rebounded on tapering the steroids down, a pre-requisite prior to a positron emission computerised tomography (PET-CT) scan to determine the source of the excess calcitriol production. This was cancelled following an emergency admission with marked hypercalcaemia and acute renal and liver injury. A contemporary CT scan showed a right apical lung mass with hepatic lesions suggestive of a disseminated lung primary. The histology obtained from a liver biopsy was compatible with metastatic small-cell lung carcinoma. Unfortunately, her clinical condition deteriorated further and she did not survive. To the best of our knowledge, this is the first report in the literature describing calcitriol-mediated hypercalcaemia due to a small-cell lung cancer.</p><p><strong>Learning points: </strong>Paraneoplastic hypercalcaemia may manifest even without overt detection of the primary cancer. The workup for paraneoplastic hypercalcaemia should be meticulous. Both bisphosphonates and steroids are useful in the initial management of calcitriol-mediated hypercalcaemia, but the definitive management is the treatment of the cause.</p>\",\"PeriodicalId\":37467,\"journal\":{\"name\":\"Endocrinology, Diabetes and Metabolism Case Reports\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/53/72/EDM22-0371.PMC10337579.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Endocrinology, Diabetes and Metabolism Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1530/EDM-22-0371\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrinology, Diabetes and Metabolism Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1530/EDM-22-0371","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
An uncanny case of paraneoplastic calcitriol mediated hypercalcaemia.
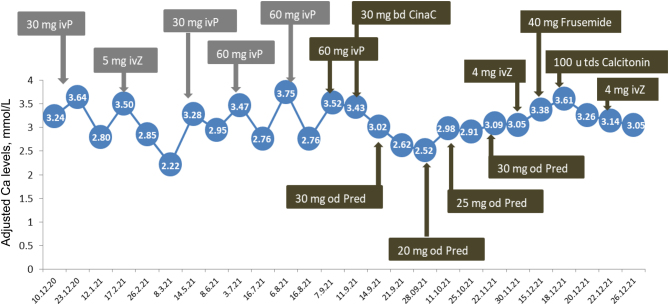
Summary: A 77-year-old female patient with a history of treated breast cancer and a recently diagnosed laryngeal cancer presented with severe hypercalcaemia associated with suppressed parathyroid hormone (PTH) levels. Her initial investigations included 25-hydroxy vitamin D levels, short synacthen test, bone scan, myeloma screen and thyroid function tests which were within normality. A computerised tomography (CT) scan showed some right lung apical fibrotic changes. Her PTH-related peptide (PTHrP) was normal and sarcoidosis was also excluded. Her previous and current malignancies were thought to be unlikely behind her hypercalcaemia. Her 1,25-dihydroxy vitamin D (calcitriol) levels were found to be elevated. Her hypercalcaemia was initially managed with intravenous fluids and intermittent bisphosphonates infusions which would transiently reduce her calcium levels. Steroid treatment was initiated which improved her hypercalcaemia; however, the calcium levels rebounded on tapering the steroids down, a pre-requisite prior to a positron emission computerised tomography (PET-CT) scan to determine the source of the excess calcitriol production. This was cancelled following an emergency admission with marked hypercalcaemia and acute renal and liver injury. A contemporary CT scan showed a right apical lung mass with hepatic lesions suggestive of a disseminated lung primary. The histology obtained from a liver biopsy was compatible with metastatic small-cell lung carcinoma. Unfortunately, her clinical condition deteriorated further and she did not survive. To the best of our knowledge, this is the first report in the literature describing calcitriol-mediated hypercalcaemia due to a small-cell lung cancer.
Learning points: Paraneoplastic hypercalcaemia may manifest even without overt detection of the primary cancer. The workup for paraneoplastic hypercalcaemia should be meticulous. Both bisphosphonates and steroids are useful in the initial management of calcitriol-mediated hypercalcaemia, but the definitive management is the treatment of the cause.
期刊介绍:
Endocrinology, Diabetes & Metabolism Case Reports publishes case reports on common and rare conditions in all areas of clinical endocrinology, diabetes and metabolism. Articles should include clear learning points which readers can use to inform medical education or clinical practice. The types of cases of interest to Endocrinology, Diabetes & Metabolism Case Reports include: -Insight into disease pathogenesis or mechanism of therapy - Novel diagnostic procedure - Novel treatment - Unique/unexpected symptoms or presentations of a disease - New disease or syndrome: presentations/diagnosis/management - Unusual effects of medical treatment - Error in diagnosis/pitfalls and caveats



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


