Agastya D Belur, Yub Raj Sedhai, Alexander G Truesdell, Ashish K Khanna, Joseph D Mishkin, P Matthew Belford, David X Zhao, Saraschandra Vallabhajosyula
{"title":"心脏骤停的目标温度管理:最新的叙述综述。","authors":"Agastya D Belur, Yub Raj Sedhai, Alexander G Truesdell, Ashish K Khanna, Joseph D Mishkin, P Matthew Belford, David X Zhao, Saraschandra Vallabhajosyula","doi":"10.1007/s40119-022-00292-4","DOIUrl":null,"url":null,"abstract":"<p><p>The established benefits of cooling along with development of sophisticated methods to safely and precisely induce, maintain, monitor, and reverse hypothermia have led to the development of targeted temperature management (TTM). Early trials in human subjects showed that hypothermia conferred better neurological outcomes when compared to normothermia among survivors of cardiac arrest, leading to guidelines recommending targeted hypothermia in this patient population. Multiple studies have sought to explore and compare the benefit of hypothermia in various subgroups of patients, such as survivors of out-of-hospital cardiac arrest versus in-hospital cardiac arrest, and survivors of an initial shockable versus non-shockable rhythm. Larger and more recent trials have shown no statistically significant difference in neurological outcomes between patients with targeted hypothermia and targeted normothermia; further, aggressive cooling is associated with a higher incidence of multiple systemic complications. Based on this data, temporal trends have leaned towards using a lenient temperature target in more recent times. Current guidelines recommend selecting and maintaining a constant target temperature between 32 and 36 °C for those patients in whom TTM is used (strong recommendation, moderate-quality evidence), as soon as possible after return of spontaneous circulation is achieved and airway, breathing (including mechanical ventilation), and circulation are stabilized. The comparative benefit of lower (32-34 °C) versus higher (36 °C) temperatures remains unknown, and further research may help elucidate this. Any survivor of cardiac arrest who is comatose (defined as unarousable unresponsiveness to external stimuli) should be considered as a candidate for TTM regardless of the initial presenting rhythm, and the decision to opt for targeted hypothermia versus targeted normothermia should be made on a case-by-case basis.</p>","PeriodicalId":9561,"journal":{"name":"Cardiology and Therapy","volume":"12 1","pages":"65-84"},"PeriodicalIF":2.7000,"publicationDate":"2023-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3b/d1/40119_2022_Article_292.PMC9986171.pdf","citationCount":"1","resultStr":"{\"title\":\"Targeted Temperature Management in Cardiac Arrest: An Updated Narrative Review.\",\"authors\":\"Agastya D Belur, Yub Raj Sedhai, Alexander G Truesdell, Ashish K Khanna, Joseph D Mishkin, P Matthew Belford, David X Zhao, Saraschandra Vallabhajosyula\",\"doi\":\"10.1007/s40119-022-00292-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The established benefits of cooling along with development of sophisticated methods to safely and precisely induce, maintain, monitor, and reverse hypothermia have led to the development of targeted temperature management (TTM). Early trials in human subjects showed that hypothermia conferred better neurological outcomes when compared to normothermia among survivors of cardiac arrest, leading to guidelines recommending targeted hypothermia in this patient population. Multiple studies have sought to explore and compare the benefit of hypothermia in various subgroups of patients, such as survivors of out-of-hospital cardiac arrest versus in-hospital cardiac arrest, and survivors of an initial shockable versus non-shockable rhythm. Larger and more recent trials have shown no statistically significant difference in neurological outcomes between patients with targeted hypothermia and targeted normothermia; further, aggressive cooling is associated with a higher incidence of multiple systemic complications. Based on this data, temporal trends have leaned towards using a lenient temperature target in more recent times. Current guidelines recommend selecting and maintaining a constant target temperature between 32 and 36 °C for those patients in whom TTM is used (strong recommendation, moderate-quality evidence), as soon as possible after return of spontaneous circulation is achieved and airway, breathing (including mechanical ventilation), and circulation are stabilized. The comparative benefit of lower (32-34 °C) versus higher (36 °C) temperatures remains unknown, and further research may help elucidate this. Any survivor of cardiac arrest who is comatose (defined as unarousable unresponsiveness to external stimuli) should be considered as a candidate for TTM regardless of the initial presenting rhythm, and the decision to opt for targeted hypothermia versus targeted normothermia should be made on a case-by-case basis.</p>\",\"PeriodicalId\":9561,\"journal\":{\"name\":\"Cardiology and Therapy\",\"volume\":\"12 1\",\"pages\":\"65-84\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2023-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3b/d1/40119_2022_Article_292.PMC9986171.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiology and Therapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s40119-022-00292-4\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology and Therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s40119-022-00292-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Targeted Temperature Management in Cardiac Arrest: An Updated Narrative Review.
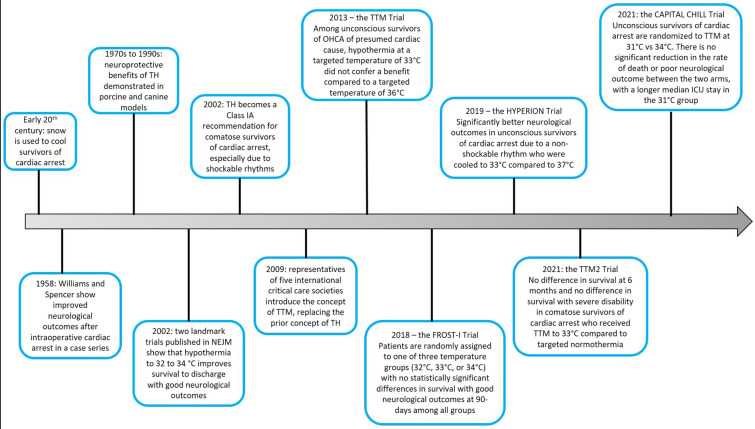
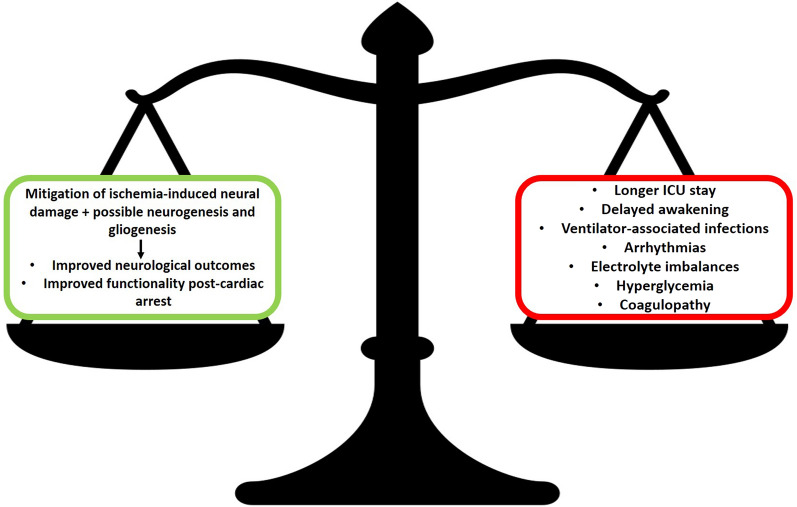
The established benefits of cooling along with development of sophisticated methods to safely and precisely induce, maintain, monitor, and reverse hypothermia have led to the development of targeted temperature management (TTM). Early trials in human subjects showed that hypothermia conferred better neurological outcomes when compared to normothermia among survivors of cardiac arrest, leading to guidelines recommending targeted hypothermia in this patient population. Multiple studies have sought to explore and compare the benefit of hypothermia in various subgroups of patients, such as survivors of out-of-hospital cardiac arrest versus in-hospital cardiac arrest, and survivors of an initial shockable versus non-shockable rhythm. Larger and more recent trials have shown no statistically significant difference in neurological outcomes between patients with targeted hypothermia and targeted normothermia; further, aggressive cooling is associated with a higher incidence of multiple systemic complications. Based on this data, temporal trends have leaned towards using a lenient temperature target in more recent times. Current guidelines recommend selecting and maintaining a constant target temperature between 32 and 36 °C for those patients in whom TTM is used (strong recommendation, moderate-quality evidence), as soon as possible after return of spontaneous circulation is achieved and airway, breathing (including mechanical ventilation), and circulation are stabilized. The comparative benefit of lower (32-34 °C) versus higher (36 °C) temperatures remains unknown, and further research may help elucidate this. Any survivor of cardiac arrest who is comatose (defined as unarousable unresponsiveness to external stimuli) should be considered as a candidate for TTM regardless of the initial presenting rhythm, and the decision to opt for targeted hypothermia versus targeted normothermia should be made on a case-by-case basis.
期刊介绍:
Aims and Scope
Cardiology and Therapy is an international, open access, peer reviewed (single-blind), rapid-publication journal dedicated to the publication of high-quality clinical (all phases), observational, real-world, and health outcomes research around the discovery, development, and use of cardiovascular therapies and interventions, including devices. Studies relating to diagnosis and diagnostics, pharmacoeconomics, public health, quality of life, as well as patient care, management and education are also encouraged.
Areas of focus include, but are not limited to, ischaemic heart disease and acute cardiac care, myocardial, valvular, pericardial and congenital heart disease, vascular and pulmonary disease (including hypertension), arrhythmias, heart failure, non-invasive diagnostic techniques, and invasive and interventional cardiology as well as cardiovascular surgery.
The journal is of interest to a broad audience of pharmaceutical and healthcare professionals and publishes original research, reviews, case reports/case series, trial protocols and short communications such as commentaries and editorials. Cardiolology and Therapy will consider all scientifically sound research be it positive, confirmatory or negative data. Submissions are welcomed whether they relate to an international and/or a country-specific audience, something that is crucially important when researchers are trying to target more specific patient populations. This inclusive approach allows the journal to assist in the dissemination of quality research, which may be considered of insufficient interest by other journals.
Rapid Publication
The journal’s publication timelines aim for a rapid peer review of 2 weeks. If an article is accepted it will be published 3–4 weeks from acceptance. The rapid timelines are achieved through the combination of a dedicated in-house editorial team, who manage article workflow, and an extensive Editorial and Advisory Board who assist with peer review. This allows the journal to support the rapid dissemination of research, whilst still providing robust peer review. Combined with the journal’s open access model this allows for the rapid, efficient communication of the latest research and reviews, fostering the advancement of cardiovascular therapies.
Personal Service
The journal’s dedicated in-house editorial team offer a personal “concierge service” meaning authors will always have an editorial contact able to update them on the status of their manuscript. The editorial team check all manuscripts to ensure that articles conform to the most recent COPE, GPP and ICMJE publishing guidelines. This supports the publication of ethically sound and transparent research.
Digital Features and Plain Language Summaries
Cardiology and Therapy offers a range of additional features designed to increase the visibility, readership and educational value of the journal’s content. Each article is accompanied by key summary points, giving a time-efficient overview of the content to a wide readership. Articles may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand the scientific content and overall implications of the article. The journal also provides the option to include various types of digital features including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations. All additional features are peer reviewed to the same high standard as the article itself. If you consider that your paper would benefit from the inclusion of a digital feature, please let us know. Our editorial team are able to create high-quality slide decks and infographics in-house, and video abstracts through our partner Research Square, and would be happy to assist in any way we can. For further information about digital features, please contact the journal editor (see ‘Contact the Journal’ for email address), and see the ‘Guidelines for digital features and plain language summaries’ document under ‘Submission guidelines’.
For examples of digital features please visit our showcase page https://springerhealthcare.com/expertise/publishing-digital-features/
Publication Fees
Upon acceptance of your article for publication, authors will be required to pay the mandatory Rapid Service Fee of £3650/€4500/$5100. The journal will consider fee discounts for developing countries and this is decided on a case by case basis.
Open Access
All articles published by Cardiology and Therapy are published open access.
Peer Review Process
Upon submission, manuscripts are assessed by the editorial team to ensure they fit within the aims and scope of the journal and are also checked for plagiarism. All suitable submissions are then subject to a comprehensive single-blind peer review. Reviewers are selected based on their relevant expertise and publication history in the subject area. The journal has an extensive pool of editorial and advisory board members who have been selected to assist with peer review based on the afore-mentioned criteria.
At least two extensive reviews are required to make the editorial decision, with the exception of some article types such as Commentaries, Editorials and Letters which are generally reviewed by one member of the Editorial Board. Where reviewer recommendations are conflicted, the editorial board will be contacted for further advice and a presiding decision. Manuscripts are then either accepted, rejected or authors are required to make major or minor revisions (both reviewer comments and editorial comments may need to be addressed). Once a revised manuscript is re-submitted, it is assessed along with the responses to reviewer comments and if it has been adequately revised it will be accepted for publication. Accepted manuscripts are then copyedited and typeset by the production team before online publication. Appeals against decisions following peer review are considered on a case by case basis and should be sent to the journal editor.
Preprints
We encourage posting of preprints of primary research manuscripts on preprint servers, authors’ or institutional websites, and open communications between researchers whether on community preprint servers or preprint commenting platforms. Posting of preprints is not considered prior publication and will not jeopardize consideration in our journals. Authors should disclose details of preprint posting during the submission process or at any other point during consideration in one of our journals. Once the preprint is published, it is the author’s responsibility to ensure that the preprint record is updated with a publication reference, including the DOI and a URL link to the published version of the article on the journal website.
Copyright
Cardiology and Therapy is published under the Creative Commons Attribution-Noncommercial License, which allows users to read, copy, distribute, and make derivative works for non-commercial purposes from the material, as long as the author of the original work is cited. The author assigns the exclusive right to any commercial use of the article to Springer. For more information about the Creative Commons Attribution-Noncommercial License, click here: http://creativecommons.org/licenses/by-nc/4.0.
Contact
For more information about the journal, including pre-submission enquiries, please contact matthew.evans@springer.com

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


