Elizabeth M Martinez, Robert J Sepanski, A Dawn Jennings, James M Schmidt, Thomas J Cholis, Meaghan E Dominy, Sanaz B Devlin, Lindsay Floyd Eilers, Arno L Zaritsky, Sandip A Godambe
{"title":"通过团队决策优化感染相关失代偿风险患者的识别和管理。","authors":"Elizabeth M Martinez, Robert J Sepanski, A Dawn Jennings, James M Schmidt, Thomas J Cholis, Meaghan E Dominy, Sanaz B Devlin, Lindsay Floyd Eilers, Arno L Zaritsky, Sandip A Godambe","doi":"10.1097/JHQ.0000000000000363","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Pediatric sepsis is a leading cause of death among children. Electronic alert systems may improve early recognition but do not consistently result in timely interventions given the multitude of clinical presentations, lack of treatment consensus, standardized order sets, and inadequate interdisciplinary team-based communication. We conducted a quality improvement project to improve timely critical treatment of patients at risk for infection-related decompensation (IRD) through team-based communication and standardized treatment workflow.</p><p><strong>Methods: </strong>We evaluated children at risk for IRD as evidenced by the activation of an electronic alert system (Children at High Risk Alert Tool [CAHR-AT]) in the emergency department. Outcomes were assessed after multiple improvements including CAHR-AT implementation, clinical coassessment, visual cues for situational awareness, huddles, and standardized order sets.</p><p><strong>Results: </strong>With visual cue activation, initial huddle compliance increased from 7.8% to 65.3% ( p < .001). Children receiving antibiotics by 3 hours postactivation increased from 37.9% pre-CAHR-AT to 50.7% posthuddle implementation ( p < .0001); patients who received a fluid bolus by 3 hours post-CAHR activation increased from 49.0% to 55.2% ( p = .001).</p><p><strong>Conclusions: </strong>Implementing a well-validated electronic alert tool did not improve quality measures of timely treatment for high-risk patients until combined with team-based communication, standardized reassessment, and treatment workflow.</p>","PeriodicalId":48801,"journal":{"name":"Journal for Healthcare Quality","volume":"45 2","pages":"59-68"},"PeriodicalIF":0.9000,"publicationDate":"2023-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0b/aa/jhq-45-59.PMC9977419.pdf","citationCount":"0","resultStr":"{\"title\":\"Optimizing Recognition and Management of Patients at Risk for Infection-Related Decompensation Through Team-Based Decision Making.\",\"authors\":\"Elizabeth M Martinez, Robert J Sepanski, A Dawn Jennings, James M Schmidt, Thomas J Cholis, Meaghan E Dominy, Sanaz B Devlin, Lindsay Floyd Eilers, Arno L Zaritsky, Sandip A Godambe\",\"doi\":\"10.1097/JHQ.0000000000000363\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Pediatric sepsis is a leading cause of death among children. Electronic alert systems may improve early recognition but do not consistently result in timely interventions given the multitude of clinical presentations, lack of treatment consensus, standardized order sets, and inadequate interdisciplinary team-based communication. We conducted a quality improvement project to improve timely critical treatment of patients at risk for infection-related decompensation (IRD) through team-based communication and standardized treatment workflow.</p><p><strong>Methods: </strong>We evaluated children at risk for IRD as evidenced by the activation of an electronic alert system (Children at High Risk Alert Tool [CAHR-AT]) in the emergency department. Outcomes were assessed after multiple improvements including CAHR-AT implementation, clinical coassessment, visual cues for situational awareness, huddles, and standardized order sets.</p><p><strong>Results: </strong>With visual cue activation, initial huddle compliance increased from 7.8% to 65.3% ( p < .001). Children receiving antibiotics by 3 hours postactivation increased from 37.9% pre-CAHR-AT to 50.7% posthuddle implementation ( p < .0001); patients who received a fluid bolus by 3 hours post-CAHR activation increased from 49.0% to 55.2% ( p = .001).</p><p><strong>Conclusions: </strong>Implementing a well-validated electronic alert tool did not improve quality measures of timely treatment for high-risk patients until combined with team-based communication, standardized reassessment, and treatment workflow.</p>\",\"PeriodicalId\":48801,\"journal\":{\"name\":\"Journal for Healthcare Quality\",\"volume\":\"45 2\",\"pages\":\"59-68\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2023-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0b/aa/jhq-45-59.PMC9977419.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal for Healthcare Quality\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1097/JHQ.0000000000000363\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal for Healthcare Quality","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/JHQ.0000000000000363","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Optimizing Recognition and Management of Patients at Risk for Infection-Related Decompensation Through Team-Based Decision Making.
Introduction: Pediatric sepsis is a leading cause of death among children. Electronic alert systems may improve early recognition but do not consistently result in timely interventions given the multitude of clinical presentations, lack of treatment consensus, standardized order sets, and inadequate interdisciplinary team-based communication. We conducted a quality improvement project to improve timely critical treatment of patients at risk for infection-related decompensation (IRD) through team-based communication and standardized treatment workflow.
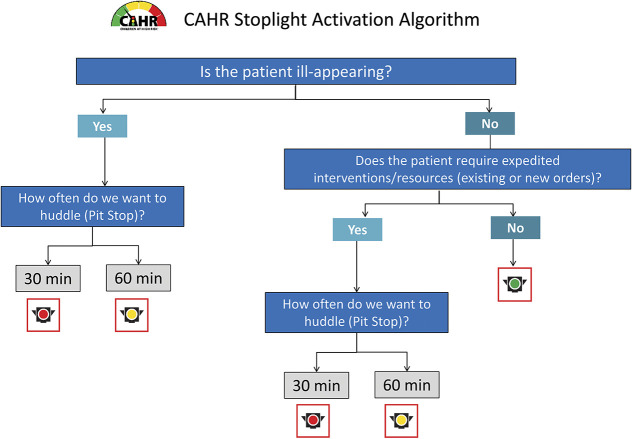
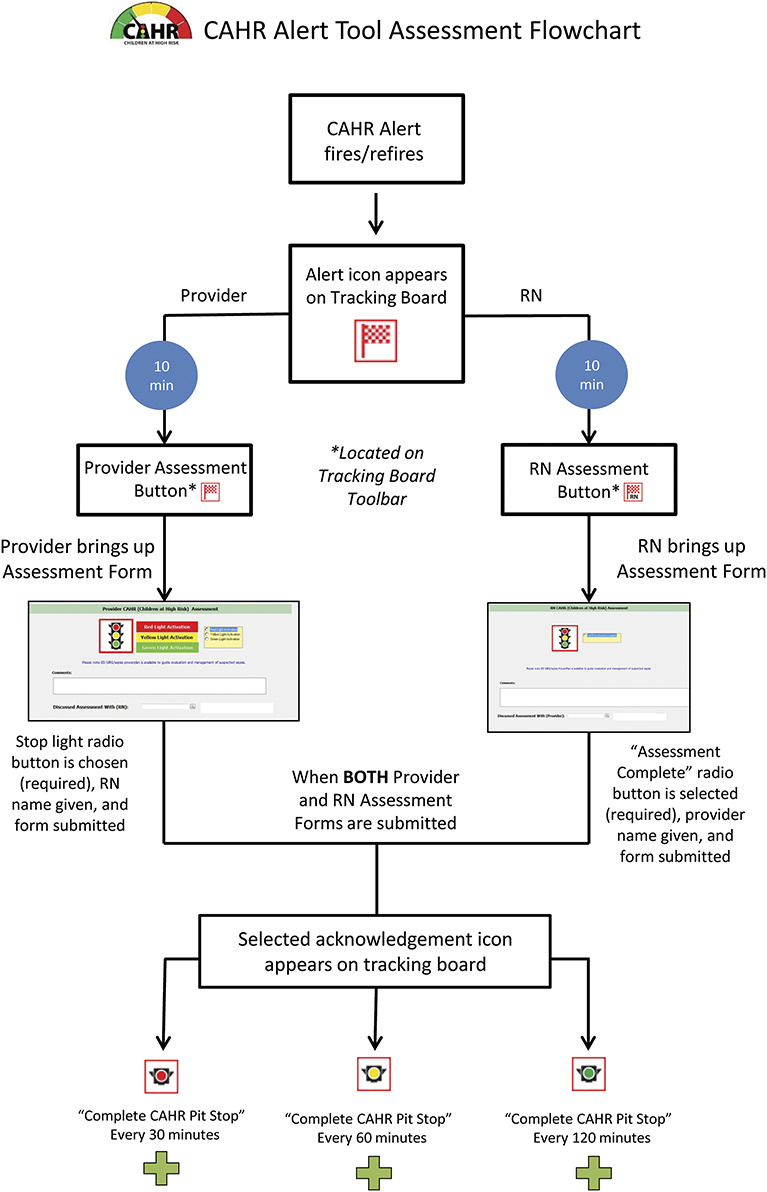
Methods: We evaluated children at risk for IRD as evidenced by the activation of an electronic alert system (Children at High Risk Alert Tool [CAHR-AT]) in the emergency department. Outcomes were assessed after multiple improvements including CAHR-AT implementation, clinical coassessment, visual cues for situational awareness, huddles, and standardized order sets.
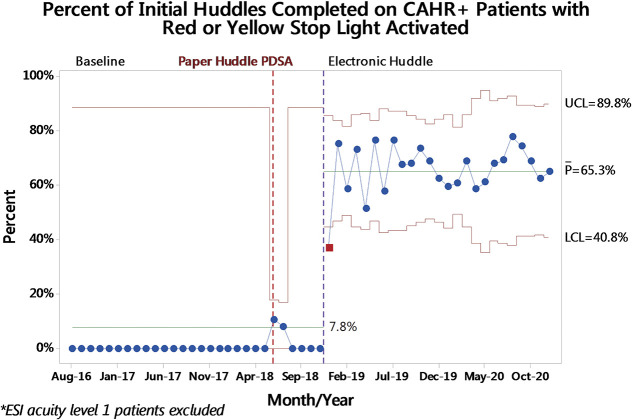
Results: With visual cue activation, initial huddle compliance increased from 7.8% to 65.3% ( p < .001). Children receiving antibiotics by 3 hours postactivation increased from 37.9% pre-CAHR-AT to 50.7% posthuddle implementation ( p < .0001); patients who received a fluid bolus by 3 hours post-CAHR activation increased from 49.0% to 55.2% ( p = .001).
Conclusions: Implementing a well-validated electronic alert tool did not improve quality measures of timely treatment for high-risk patients until combined with team-based communication, standardized reassessment, and treatment workflow.
期刊介绍:
The Journal for Healthcare Quality (JHQ), a peer-reviewed journal, is an official publication of the National Association for Healthcare Quality. JHQ is a professional forum that continuously advances healthcare quality practice in diverse and changing environments, and is the first choice for creative and scientific solutions in the pursuit of healthcare quality. It has been selected for coverage in Thomson Reuter’s Science Citation Index Expanded, Social Sciences Citation Index®, and Current Contents®.
The Journal publishes scholarly articles that are targeted to leaders of all healthcare settings, leveraging applied research and producing practical, timely and impactful evidence in healthcare system transformation. The journal covers topics such as:
Quality Improvement • Patient Safety • Performance Measurement • Best Practices in Clinical and Operational Processes • Innovation • Leadership • Information Technology • Spreading Improvement • Sustaining Improvement • Cost Reduction • Payment Reform

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


