{"title":"动脉瘤性蛛网膜下腔出血栓塞后出现动脉瘤内血栓并延迟线圈移位:一个例证性病例。","authors":"Koichiro Suzuki, Kazunori Oda, Yoshinobu Horio, Dai Kawano, Noriko Hirao, Takaaki Amamoto, Hiromasa Kobayashi, Koichiro Takemoto, Takashi Morishita, Hiroshi Abe","doi":"10.3171/CASE23196","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Coil migration is a rare, but notable complication of endovascular treatment. Risk factors include communicating segment aneurysms, aneurysmal shape, and technical factors. Although cerebral blood flow obstruction caused by early coil migration requires urgent coil removal, delayed coil migration is often asymptomatic, making it difficult to determine a treatment strategy.</p><p><strong>Observations: </strong>A 47-year-old woman was referred to the institute with acute-onset headache. She was diagnosed with subarachnoid hemorrhage due to rupture of the right internal carotid artery-posterior communicating artery aneurysm and underwent endovascular coil embolization. Following the procedure, the patient showed no obvious complications; however, 14 days later, images showed coil migration to the distal side, leading to surgical removal. Right frontotemporal craniotomy was performed, and the remaining coil was removed. The aneurysm was clipped again, and blood flow was confirmed. The patient was discharged 12 days after the craniotomy with transient oculomotor nerve palsy. At the 15-month follow-up, there was no aneurysm recurrence and the oculomotor nerve palsy showed improvement.</p><p><strong>Lessons: </strong>Retrieval of the migrated coil by craniotomy is an effective remedial measure; however, intraoperative complications are common. Early detection, established protocols, and prompt treatment decisions are important for preventing undesirable outcomes.</p>","PeriodicalId":16554,"journal":{"name":"Journal of Neurosurgery: Case Lessons","volume":"5 26","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-06-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/50/00/CASE23196.PMC10550549.pdf","citationCount":"0","resultStr":"{\"title\":\"Presence of intra-aneurysmal thrombi with delayed coil migration after embolization of an aneurysmal subarachnoid hemorrhage: illustrative case.\",\"authors\":\"Koichiro Suzuki, Kazunori Oda, Yoshinobu Horio, Dai Kawano, Noriko Hirao, Takaaki Amamoto, Hiromasa Kobayashi, Koichiro Takemoto, Takashi Morishita, Hiroshi Abe\",\"doi\":\"10.3171/CASE23196\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Coil migration is a rare, but notable complication of endovascular treatment. Risk factors include communicating segment aneurysms, aneurysmal shape, and technical factors. Although cerebral blood flow obstruction caused by early coil migration requires urgent coil removal, delayed coil migration is often asymptomatic, making it difficult to determine a treatment strategy.</p><p><strong>Observations: </strong>A 47-year-old woman was referred to the institute with acute-onset headache. She was diagnosed with subarachnoid hemorrhage due to rupture of the right internal carotid artery-posterior communicating artery aneurysm and underwent endovascular coil embolization. Following the procedure, the patient showed no obvious complications; however, 14 days later, images showed coil migration to the distal side, leading to surgical removal. Right frontotemporal craniotomy was performed, and the remaining coil was removed. The aneurysm was clipped again, and blood flow was confirmed. The patient was discharged 12 days after the craniotomy with transient oculomotor nerve palsy. At the 15-month follow-up, there was no aneurysm recurrence and the oculomotor nerve palsy showed improvement.</p><p><strong>Lessons: </strong>Retrieval of the migrated coil by craniotomy is an effective remedial measure; however, intraoperative complications are common. Early detection, established protocols, and prompt treatment decisions are important for preventing undesirable outcomes.</p>\",\"PeriodicalId\":16554,\"journal\":{\"name\":\"Journal of Neurosurgery: Case Lessons\",\"volume\":\"5 26\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-06-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/50/00/CASE23196.PMC10550549.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Neurosurgery: Case Lessons\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3171/CASE23196\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neurosurgery: Case Lessons","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3171/CASE23196","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Presence of intra-aneurysmal thrombi with delayed coil migration after embolization of an aneurysmal subarachnoid hemorrhage: illustrative case.
Background: Coil migration is a rare, but notable complication of endovascular treatment. Risk factors include communicating segment aneurysms, aneurysmal shape, and technical factors. Although cerebral blood flow obstruction caused by early coil migration requires urgent coil removal, delayed coil migration is often asymptomatic, making it difficult to determine a treatment strategy.
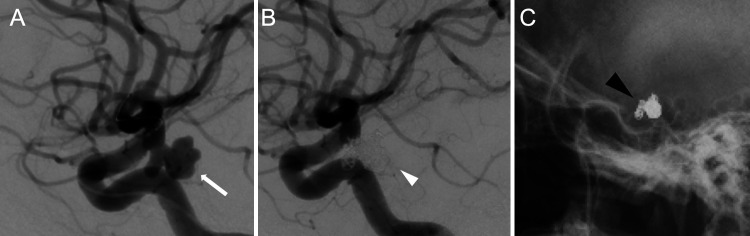
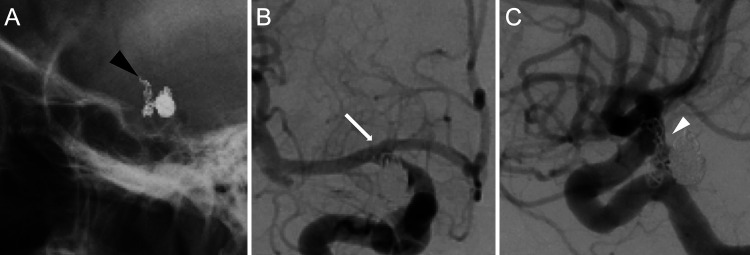
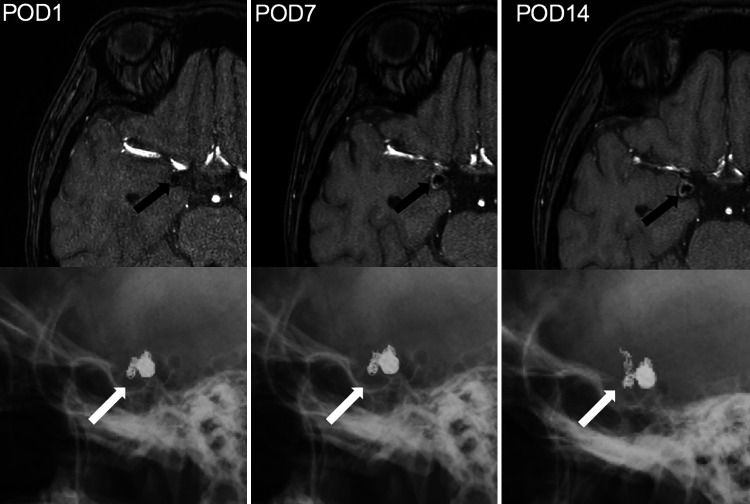
Observations: A 47-year-old woman was referred to the institute with acute-onset headache. She was diagnosed with subarachnoid hemorrhage due to rupture of the right internal carotid artery-posterior communicating artery aneurysm and underwent endovascular coil embolization. Following the procedure, the patient showed no obvious complications; however, 14 days later, images showed coil migration to the distal side, leading to surgical removal. Right frontotemporal craniotomy was performed, and the remaining coil was removed. The aneurysm was clipped again, and blood flow was confirmed. The patient was discharged 12 days after the craniotomy with transient oculomotor nerve palsy. At the 15-month follow-up, there was no aneurysm recurrence and the oculomotor nerve palsy showed improvement.
Lessons: Retrieval of the migrated coil by craniotomy is an effective remedial measure; however, intraoperative complications are common. Early detection, established protocols, and prompt treatment decisions are important for preventing undesirable outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


