Jason George, Daniel White, Barbara Fielding, Michael Scott, Timothy Rockall, Martin Brunel Whyte
{"title":"大胃肠手术术前n-3脂肪酸的系统评价。","authors":"Jason George, Daniel White, Barbara Fielding, Michael Scott, Timothy Rockall, Martin Brunel Whyte","doi":"10.1136/bmjsit-2022-000172","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Perioperative nutrition aims to replenish nutritional stores before surgery and reduce postoperative complications. 'Immunonutrition' (including omega-3 fatty acids) may modulate the immune system and attenuate the postoperative inflammatory response. Hitherto, immunonutrition has overwhelmingly been administered in the postoperative period-however, this may be too late to provide benefit.</p><p><strong>Design: </strong>A systematic literature search using MEDLINE and EMBASE for randomized controlled trials (RCTs).</p><p><strong>Setting: </strong>Perioperative major gastrointestinal surgery.</p><p><strong>Participants: </strong>Patients undergoing major gastrointestinal surgery.</p><p><strong>Interventions: </strong>Omega-3 fatty acid supplementation commenced in the preoperative period, with or without continuation into postoperative period.</p><p><strong>Main outcome measures: </strong>The effect of preoperative omega-3 fatty acids on inflammatory response and clinical outcomes.</p><p><strong>Results: </strong>833 studies were identified. After applying inclusion and exclusion criteria, 12 RCTs, involving 1456 randomized patients, were included. Ten articles exclusively enrolled patients with cancer. Seven studies used a combination of EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid) as the intervention and five studies used EPA alone. Eight out of 12 studies continued preoperative nutritional support into the postoperative period.Of the nine studies reporting mortality, no difference was seen. Duration of hospitalisation ranged from 4.5 to 18 days with intervention and 3.5 to 23.5 days with control. Omega-3 fatty acids had no effect on postoperative C-reactive protein and the effect on cytokines (including tumor necrosis factor-α, interleukin (IL)-6 and IL-10) was inconsistent. Ten of the 12 studies had low risk of bias, with one study having moderate bias from allocation and blinding.</p><p><strong>Conclusions: </strong>There is insufficient evidence to support routine preoperative omega-3 fatty acid supplementation for major gastrointestinal surgery, even when this is continued after surgery.</p><p><strong>Prospero registration number: </strong>CRD42018108333.</p>","PeriodicalId":33349,"journal":{"name":"BMJ Surgery Interventions Health Technologies","volume":"5 1","pages":"e000172"},"PeriodicalIF":1.6000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/18/3d/bmjsit-2022-000172.PMC10314636.pdf","citationCount":"0","resultStr":"{\"title\":\"Systematic review of preoperative n-3 fatty acids in major gastrointestinal surgery.\",\"authors\":\"Jason George, Daniel White, Barbara Fielding, Michael Scott, Timothy Rockall, Martin Brunel Whyte\",\"doi\":\"10.1136/bmjsit-2022-000172\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Perioperative nutrition aims to replenish nutritional stores before surgery and reduce postoperative complications. 'Immunonutrition' (including omega-3 fatty acids) may modulate the immune system and attenuate the postoperative inflammatory response. Hitherto, immunonutrition has overwhelmingly been administered in the postoperative period-however, this may be too late to provide benefit.</p><p><strong>Design: </strong>A systematic literature search using MEDLINE and EMBASE for randomized controlled trials (RCTs).</p><p><strong>Setting: </strong>Perioperative major gastrointestinal surgery.</p><p><strong>Participants: </strong>Patients undergoing major gastrointestinal surgery.</p><p><strong>Interventions: </strong>Omega-3 fatty acid supplementation commenced in the preoperative period, with or without continuation into postoperative period.</p><p><strong>Main outcome measures: </strong>The effect of preoperative omega-3 fatty acids on inflammatory response and clinical outcomes.</p><p><strong>Results: </strong>833 studies were identified. After applying inclusion and exclusion criteria, 12 RCTs, involving 1456 randomized patients, were included. Ten articles exclusively enrolled patients with cancer. Seven studies used a combination of EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid) as the intervention and five studies used EPA alone. Eight out of 12 studies continued preoperative nutritional support into the postoperative period.Of the nine studies reporting mortality, no difference was seen. Duration of hospitalisation ranged from 4.5 to 18 days with intervention and 3.5 to 23.5 days with control. Omega-3 fatty acids had no effect on postoperative C-reactive protein and the effect on cytokines (including tumor necrosis factor-α, interleukin (IL)-6 and IL-10) was inconsistent. Ten of the 12 studies had low risk of bias, with one study having moderate bias from allocation and blinding.</p><p><strong>Conclusions: </strong>There is insufficient evidence to support routine preoperative omega-3 fatty acid supplementation for major gastrointestinal surgery, even when this is continued after surgery.</p><p><strong>Prospero registration number: </strong>CRD42018108333.</p>\",\"PeriodicalId\":33349,\"journal\":{\"name\":\"BMJ Surgery Interventions Health Technologies\",\"volume\":\"5 1\",\"pages\":\"e000172\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/18/3d/bmjsit-2022-000172.PMC10314636.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Surgery Interventions Health Technologies\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjsit-2022-000172\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Surgery Interventions Health Technologies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjsit-2022-000172","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
Systematic review of preoperative n-3 fatty acids in major gastrointestinal surgery.
Objectives: Perioperative nutrition aims to replenish nutritional stores before surgery and reduce postoperative complications. 'Immunonutrition' (including omega-3 fatty acids) may modulate the immune system and attenuate the postoperative inflammatory response. Hitherto, immunonutrition has overwhelmingly been administered in the postoperative period-however, this may be too late to provide benefit.
Design: A systematic literature search using MEDLINE and EMBASE for randomized controlled trials (RCTs).
Setting: Perioperative major gastrointestinal surgery.
Participants: Patients undergoing major gastrointestinal surgery.
Interventions: Omega-3 fatty acid supplementation commenced in the preoperative period, with or without continuation into postoperative period.
Main outcome measures: The effect of preoperative omega-3 fatty acids on inflammatory response and clinical outcomes.
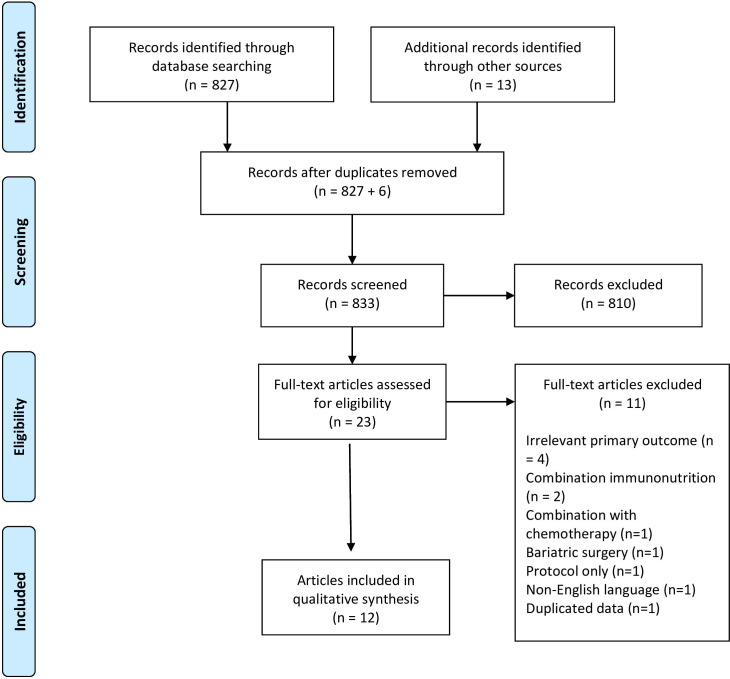
Results: 833 studies were identified. After applying inclusion and exclusion criteria, 12 RCTs, involving 1456 randomized patients, were included. Ten articles exclusively enrolled patients with cancer. Seven studies used a combination of EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid) as the intervention and five studies used EPA alone. Eight out of 12 studies continued preoperative nutritional support into the postoperative period.Of the nine studies reporting mortality, no difference was seen. Duration of hospitalisation ranged from 4.5 to 18 days with intervention and 3.5 to 23.5 days with control. Omega-3 fatty acids had no effect on postoperative C-reactive protein and the effect on cytokines (including tumor necrosis factor-α, interleukin (IL)-6 and IL-10) was inconsistent. Ten of the 12 studies had low risk of bias, with one study having moderate bias from allocation and blinding.
Conclusions: There is insufficient evidence to support routine preoperative omega-3 fatty acid supplementation for major gastrointestinal surgery, even when this is continued after surgery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


