Ozgur Surgit, Ahmet Güner, İrem Türkmen, Serkan Kahraman, Nail Guven Serbest, Ezgi Gültekin Güner, Fatih Uzun, Mehmet Ertürk, Mustafa Yildiz
{"title":"中高风险肺栓塞患者的低剂量溶栓治疗与未分割肝素治疗。","authors":"Ozgur Surgit, Ahmet Güner, İrem Türkmen, Serkan Kahraman, Nail Guven Serbest, Ezgi Gültekin Güner, Fatih Uzun, Mehmet Ertürk, Mustafa Yildiz","doi":"10.14744/tjtes.2023.55236","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with intermediate-high risk pulmonary embolism (PE) who have acute right ventricular dysfunction and myocardial injury without overt hemodynamic compromise may be candidates for thrombolytic therapy (TT). In this study, we aimed to compare the clinical outcomes of low-dose prolonged TT and unfractionated heparin (UFH) in intermediate-high risk PE patients.</p><p><strong>Methods: </strong>This study enrolled 83 (female: 45 [54.2%], mean age: 70.07±10.7 years) retrospectively evaluated patients with the diagnosis of acute PE who were treated with low-dose and slow-infusion of TT or UFH. The primary outcomes of the study were de-fined as a combination of death from any cause and hemodynamic decompensation, and severe or life-threatening bleeding. Secondary endpoints were recurrent PE, pulmonary hypertension, and moderate bleeding.</p><p><strong>Results: </strong>The initial management strategy of intermediate-high risk PE was TT in 41 (49.4%) patients and UFH in 42 (50.6%) cases. Low-dose prolonged TT was successful in all patients. While the frequency of hypotension decreased significantly after TT (22 vs. 0%, P<0.001), it did not decrease after UFH (2.4 vs. 7.1%, p=0.625). The proportion of hemodynamic decompensation was significantly lower in the TT group (0 vs. 11.9%, p=0.029). The rate of secondary endpoints was significantly higher in the UFH group (2.4 vs. 19%, P=0.016). Moreover, the prevalence of pulmonary hypertension was significantly higher in UFH group (0 vs. 19%, p=0.003).</p><p><strong>Conclusion: </strong>Prolonged TT regimen with low dose, slow infusion of tissue plasminogen activator was found to be associated with a lower risk of hemodynamic decompensation and pulmonary hypertension in patients with acute intermediate-high-risk PE compared to UFH.</p>","PeriodicalId":49398,"journal":{"name":"Ulusal Travma Ve Acil Cerrahi Dergisi-Turkish Journal of Trauma & Emergency Surgery","volume":"29 6","pages":"677-684"},"PeriodicalIF":0.8000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/af/6e/TJTES-29-677.PMC10315937.pdf","citationCount":"0","resultStr":"{\"title\":\"Low-dose thrombolytic therapy versus unfractionated heparin in patients with intermediate-high risk pulmonary embolism.\",\"authors\":\"Ozgur Surgit, Ahmet Güner, İrem Türkmen, Serkan Kahraman, Nail Guven Serbest, Ezgi Gültekin Güner, Fatih Uzun, Mehmet Ertürk, Mustafa Yildiz\",\"doi\":\"10.14744/tjtes.2023.55236\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Patients with intermediate-high risk pulmonary embolism (PE) who have acute right ventricular dysfunction and myocardial injury without overt hemodynamic compromise may be candidates for thrombolytic therapy (TT). In this study, we aimed to compare the clinical outcomes of low-dose prolonged TT and unfractionated heparin (UFH) in intermediate-high risk PE patients.</p><p><strong>Methods: </strong>This study enrolled 83 (female: 45 [54.2%], mean age: 70.07±10.7 years) retrospectively evaluated patients with the diagnosis of acute PE who were treated with low-dose and slow-infusion of TT or UFH. The primary outcomes of the study were de-fined as a combination of death from any cause and hemodynamic decompensation, and severe or life-threatening bleeding. Secondary endpoints were recurrent PE, pulmonary hypertension, and moderate bleeding.</p><p><strong>Results: </strong>The initial management strategy of intermediate-high risk PE was TT in 41 (49.4%) patients and UFH in 42 (50.6%) cases. Low-dose prolonged TT was successful in all patients. While the frequency of hypotension decreased significantly after TT (22 vs. 0%, P<0.001), it did not decrease after UFH (2.4 vs. 7.1%, p=0.625). The proportion of hemodynamic decompensation was significantly lower in the TT group (0 vs. 11.9%, p=0.029). The rate of secondary endpoints was significantly higher in the UFH group (2.4 vs. 19%, P=0.016). Moreover, the prevalence of pulmonary hypertension was significantly higher in UFH group (0 vs. 19%, p=0.003).</p><p><strong>Conclusion: </strong>Prolonged TT regimen with low dose, slow infusion of tissue plasminogen activator was found to be associated with a lower risk of hemodynamic decompensation and pulmonary hypertension in patients with acute intermediate-high-risk PE compared to UFH.</p>\",\"PeriodicalId\":49398,\"journal\":{\"name\":\"Ulusal Travma Ve Acil Cerrahi Dergisi-Turkish Journal of Trauma & Emergency Surgery\",\"volume\":\"29 6\",\"pages\":\"677-684\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/af/6e/TJTES-29-677.PMC10315937.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Ulusal Travma Ve Acil Cerrahi Dergisi-Turkish Journal of Trauma & Emergency Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.14744/tjtes.2023.55236\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ulusal Travma Ve Acil Cerrahi Dergisi-Turkish Journal of Trauma & Emergency Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14744/tjtes.2023.55236","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Low-dose thrombolytic therapy versus unfractionated heparin in patients with intermediate-high risk pulmonary embolism.
Background: Patients with intermediate-high risk pulmonary embolism (PE) who have acute right ventricular dysfunction and myocardial injury without overt hemodynamic compromise may be candidates for thrombolytic therapy (TT). In this study, we aimed to compare the clinical outcomes of low-dose prolonged TT and unfractionated heparin (UFH) in intermediate-high risk PE patients.
Methods: This study enrolled 83 (female: 45 [54.2%], mean age: 70.07±10.7 years) retrospectively evaluated patients with the diagnosis of acute PE who were treated with low-dose and slow-infusion of TT or UFH. The primary outcomes of the study were de-fined as a combination of death from any cause and hemodynamic decompensation, and severe or life-threatening bleeding. Secondary endpoints were recurrent PE, pulmonary hypertension, and moderate bleeding.
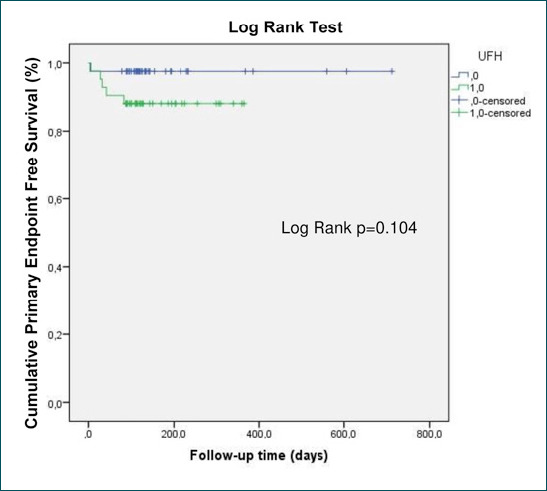
Results: The initial management strategy of intermediate-high risk PE was TT in 41 (49.4%) patients and UFH in 42 (50.6%) cases. Low-dose prolonged TT was successful in all patients. While the frequency of hypotension decreased significantly after TT (22 vs. 0%, P<0.001), it did not decrease after UFH (2.4 vs. 7.1%, p=0.625). The proportion of hemodynamic decompensation was significantly lower in the TT group (0 vs. 11.9%, p=0.029). The rate of secondary endpoints was significantly higher in the UFH group (2.4 vs. 19%, P=0.016). Moreover, the prevalence of pulmonary hypertension was significantly higher in UFH group (0 vs. 19%, p=0.003).
Conclusion: Prolonged TT regimen with low dose, slow infusion of tissue plasminogen activator was found to be associated with a lower risk of hemodynamic decompensation and pulmonary hypertension in patients with acute intermediate-high-risk PE compared to UFH.
期刊介绍:
The Turkish Journal of Trauma and Emergency Surgery (TJTES) is an official publication of the Turkish Association of Trauma and Emergency Surgery. It is a double-blind and peer-reviewed periodical that considers for publication clinical and experimental studies, case reports, technical contributions, and letters to the editor. Scope of the journal covers the trauma and emergency surgery.
Each submission will be reviewed by at least two external, independent peer reviewers who are experts in their fields in order to ensure an unbiased evaluation process. The editorial board will invite an external and independent reviewer to manage the evaluation processes of manuscripts submitted by editors or by the editorial board members of the journal. The Editor in Chief is the final authority in the decision-making process for all submissions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


