Yuefeng Hou, Leah P Griffin, Kari Ertmer, Stéphanie F Bernatchez, Tarja J Kärpänen, Maria Palka-Santini
{"title":"在COVID-19期间,静脉接入点消毒帽在减少中心静脉相关血流感染、临床使用和护理成本方面的有效性","authors":"Yuefeng Hou, Leah P Griffin, Kari Ertmer, Stéphanie F Bernatchez, Tarja J Kärpänen, Maria Palka-Santini","doi":"10.2147/CEOR.S404823","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Intravenous (IV) access point protectors, serving as passive disinfection devices and a cover between line accesses, are available to help reduce the risk of central line-associated bloodstream infections (CLABSIs). This low-maintenance disinfection solution is particularly valuable in situations with excessive workloads. This study examined the effect of a disinfecting cap for an IV access point on CLABSI rates, hospital length of stay, and cost of care in an inpatient setting during the coronavirus disease 2019 (COVID-19) pandemic.</p><p><strong>Methods: </strong>The study utilized data from the Premier Healthcare Database, focusing on 200,411 hospitalizations involving central venous catheters between January 2020 and September 2020. Among these cases, 7423 patients received a disinfecting cap, while 192,988 patients did not use any disinfecting caps and followed the standard practice of hub scrubbing. The two cohorts, Disinfecting Cap and No-Disinfecting Cap groups, were compared in terms of CLABSI rates, hospital length of stay (LOS), and hospitalization costs. The analysis accounted for baseline group differences and random clustering effects by employing a 34-variable propensity score and mixed-effect multiple regression, respectively.</p><p><strong>Results: </strong>The findings demonstrated a significant 73% decrease in CLABSI rates (p= 0.0013) in the Disinfecting Cap group, with an adjusted CLABSI rate of 0.3% compared to 1.1% in the No-Disinfecting Cap group. Additionally, the Disinfecting Cap group exhibited a 0.5-day reduction in hospital stay (9.2 days versus 9.7 days; p = 0.0169) and cost savings of $6703 ($35,604 versus $42,307; p = 0.0063) per hospital stay compared to the No-Disinfecting Cap group.</p><p><strong>Conclusion: </strong>This study provides real-world evidence that implementing a disinfecting cap to protect IV access points effectively reduces the risk of CLABSIs in hospitalized patients compared to standard care, ultimately optimizing the utilization of healthcare resources, particularly in situations where the healthcare system is under significant strain or overloaded.</p>","PeriodicalId":47313,"journal":{"name":"ClinicoEconomics and Outcomes Research","volume":"15 ","pages":"477-486"},"PeriodicalIF":2.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7f/73/ceor-15-477.PMC10290837.pdf","citationCount":"0","resultStr":"{\"title\":\"Effectiveness of Disinfecting Caps for Intravenous Access Points in Reducing Central Line-Associated Bloodstream Infections, Clinical Utilization, and Cost of Care During COVID-19.\",\"authors\":\"Yuefeng Hou, Leah P Griffin, Kari Ertmer, Stéphanie F Bernatchez, Tarja J Kärpänen, Maria Palka-Santini\",\"doi\":\"10.2147/CEOR.S404823\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Intravenous (IV) access point protectors, serving as passive disinfection devices and a cover between line accesses, are available to help reduce the risk of central line-associated bloodstream infections (CLABSIs). This low-maintenance disinfection solution is particularly valuable in situations with excessive workloads. This study examined the effect of a disinfecting cap for an IV access point on CLABSI rates, hospital length of stay, and cost of care in an inpatient setting during the coronavirus disease 2019 (COVID-19) pandemic.</p><p><strong>Methods: </strong>The study utilized data from the Premier Healthcare Database, focusing on 200,411 hospitalizations involving central venous catheters between January 2020 and September 2020. Among these cases, 7423 patients received a disinfecting cap, while 192,988 patients did not use any disinfecting caps and followed the standard practice of hub scrubbing. The two cohorts, Disinfecting Cap and No-Disinfecting Cap groups, were compared in terms of CLABSI rates, hospital length of stay (LOS), and hospitalization costs. The analysis accounted for baseline group differences and random clustering effects by employing a 34-variable propensity score and mixed-effect multiple regression, respectively.</p><p><strong>Results: </strong>The findings demonstrated a significant 73% decrease in CLABSI rates (p= 0.0013) in the Disinfecting Cap group, with an adjusted CLABSI rate of 0.3% compared to 1.1% in the No-Disinfecting Cap group. Additionally, the Disinfecting Cap group exhibited a 0.5-day reduction in hospital stay (9.2 days versus 9.7 days; p = 0.0169) and cost savings of $6703 ($35,604 versus $42,307; p = 0.0063) per hospital stay compared to the No-Disinfecting Cap group.</p><p><strong>Conclusion: </strong>This study provides real-world evidence that implementing a disinfecting cap to protect IV access points effectively reduces the risk of CLABSIs in hospitalized patients compared to standard care, ultimately optimizing the utilization of healthcare resources, particularly in situations where the healthcare system is under significant strain or overloaded.</p>\",\"PeriodicalId\":47313,\"journal\":{\"name\":\"ClinicoEconomics and Outcomes Research\",\"volume\":\"15 \",\"pages\":\"477-486\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7f/73/ceor-15-477.PMC10290837.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ClinicoEconomics and Outcomes Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/CEOR.S404823\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ClinicoEconomics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEOR.S404823","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Effectiveness of Disinfecting Caps for Intravenous Access Points in Reducing Central Line-Associated Bloodstream Infections, Clinical Utilization, and Cost of Care During COVID-19.
Purpose: Intravenous (IV) access point protectors, serving as passive disinfection devices and a cover between line accesses, are available to help reduce the risk of central line-associated bloodstream infections (CLABSIs). This low-maintenance disinfection solution is particularly valuable in situations with excessive workloads. This study examined the effect of a disinfecting cap for an IV access point on CLABSI rates, hospital length of stay, and cost of care in an inpatient setting during the coronavirus disease 2019 (COVID-19) pandemic.
Methods: The study utilized data from the Premier Healthcare Database, focusing on 200,411 hospitalizations involving central venous catheters between January 2020 and September 2020. Among these cases, 7423 patients received a disinfecting cap, while 192,988 patients did not use any disinfecting caps and followed the standard practice of hub scrubbing. The two cohorts, Disinfecting Cap and No-Disinfecting Cap groups, were compared in terms of CLABSI rates, hospital length of stay (LOS), and hospitalization costs. The analysis accounted for baseline group differences and random clustering effects by employing a 34-variable propensity score and mixed-effect multiple regression, respectively.
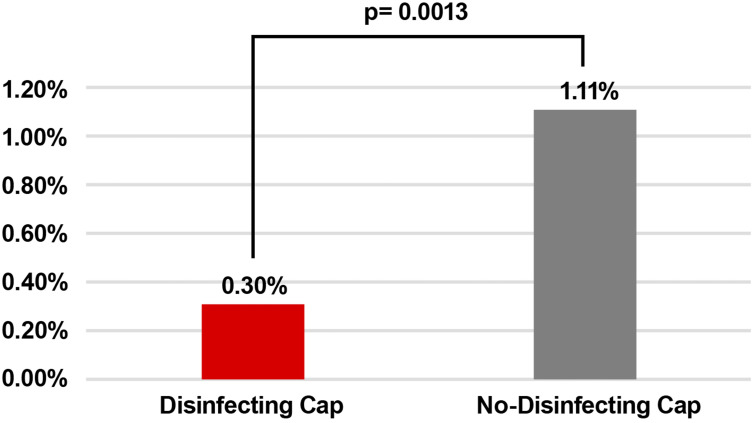
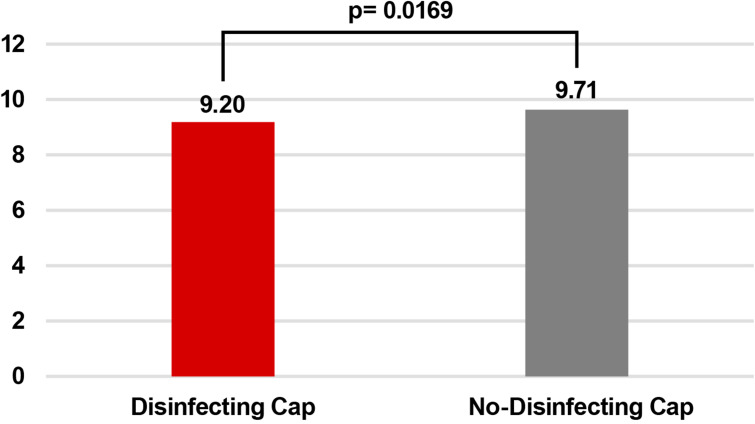
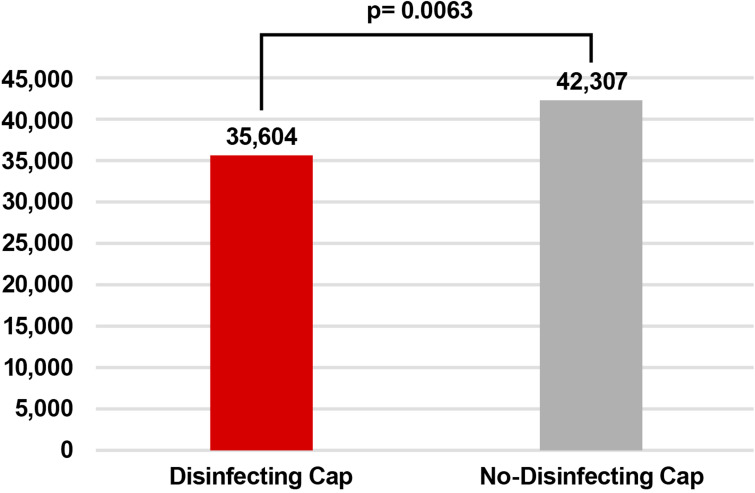
Results: The findings demonstrated a significant 73% decrease in CLABSI rates (p= 0.0013) in the Disinfecting Cap group, with an adjusted CLABSI rate of 0.3% compared to 1.1% in the No-Disinfecting Cap group. Additionally, the Disinfecting Cap group exhibited a 0.5-day reduction in hospital stay (9.2 days versus 9.7 days; p = 0.0169) and cost savings of $6703 ($35,604 versus $42,307; p = 0.0063) per hospital stay compared to the No-Disinfecting Cap group.
Conclusion: This study provides real-world evidence that implementing a disinfecting cap to protect IV access points effectively reduces the risk of CLABSIs in hospitalized patients compared to standard care, ultimately optimizing the utilization of healthcare resources, particularly in situations where the healthcare system is under significant strain or overloaded.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


