Osama Alhadramy, Refal A Alahmadi, Afrah M Alameen, Nada S Ashmawi, Nadeen A Alrehaili, Rahaf A Afandi, Tahani A Alrehaili, Saba Kassim
{"title":"新发心力衰竭保留和降低门诊患者射血分数的区别特征和治疗反应。","authors":"Osama Alhadramy, Refal A Alahmadi, Afrah M Alameen, Nada S Ashmawi, Nadeen A Alrehaili, Rahaf A Afandi, Tahani A Alrehaili, Saba Kassim","doi":"10.14740/cr1483","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Differences in clinical presentation and therapy outcomes between heart failure with preserved ejection fraction (HFpEF) and heart failure with reduced ejection fraction (HFrEF) have been reported but described mainly among hospitalized patients. Because the population of outpatients with heart failure (HF) is increasing, we sought to discriminate the clinical presentation and responses to medical therapy in ambulatory patients with new-onset HFpEF vs. HFrEF.</p><p><strong>Methods: </strong>We retrospectively included all patients with new-onset HF treated at a single HF clinic in the past 4 years. Clinical data and electrocardiography (ECG) and echocardiography findings were recorded. Patients were followed up once weekly, and treatment response was evaluated according to symptoms resolution within 30 days. Univariate and multivariate regression analyses were performed.</p><p><strong>Results: </strong>A total of 146 patients were diagnosed with new-onset HF: 68 with HFpEF and 78 with HFrEF. The patients with HFrEF were older than those with HFpEF (66.9 vs. 62 years, respectively, P = 0.008). Patients with HFrEF were more likely to have coronary artery disease, atrial fibrillation, or valvular heart disease than those with HFpEF (P < 0.05 for all). Patients with HFrEF rather than HFpEF were more likely to present with New York Heart Association class 3 - 4 dyspnea, orthopnea, paroxysmal nocturnal dyspnea or low cardiac output (P < 0.007 for all). Patients with HFpEF were more likely than those with HFpEF to have normal ECG at presentation (P < 0.001), and left bundle branch block (LBBB) was observed only in patients with HFrEF (P < 0.001). Resolution of symptoms within 30 days occurred in 75% of patients with HFpEF and 40% of patients with HFrEF (P < 0.001).</p><p><strong>Conclusions: </strong>Ambulatory patients with new-onset HFrEF were older, and had higher incidence of structural heart disease, in comparison to those with new-onset HFpEF. Patients presenting with HFrEF had more severe functional symptoms than those with HFpEF. Patients with HFpEF were more likely than those with HFpEF to have normal ECG at the time of presentation, and LBBB was strongly associated with HFrEF. Outpatients with HFrEF rather than HFpEF were less likely to respond to treatment.</p>","PeriodicalId":9424,"journal":{"name":"Cardiology Research","volume":"14 3","pages":"201-210"},"PeriodicalIF":1.4000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9f/82/cr-14-201.PMC10257507.pdf","citationCount":"0","resultStr":"{\"title\":\"Differentiating Characteristics and Responses to Treatment of New-Onset Heart Failure With Preserved and Reduced Ejection Fraction in Ambulatory Patients.\",\"authors\":\"Osama Alhadramy, Refal A Alahmadi, Afrah M Alameen, Nada S Ashmawi, Nadeen A Alrehaili, Rahaf A Afandi, Tahani A Alrehaili, Saba Kassim\",\"doi\":\"10.14740/cr1483\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Differences in clinical presentation and therapy outcomes between heart failure with preserved ejection fraction (HFpEF) and heart failure with reduced ejection fraction (HFrEF) have been reported but described mainly among hospitalized patients. Because the population of outpatients with heart failure (HF) is increasing, we sought to discriminate the clinical presentation and responses to medical therapy in ambulatory patients with new-onset HFpEF vs. HFrEF.</p><p><strong>Methods: </strong>We retrospectively included all patients with new-onset HF treated at a single HF clinic in the past 4 years. Clinical data and electrocardiography (ECG) and echocardiography findings were recorded. Patients were followed up once weekly, and treatment response was evaluated according to symptoms resolution within 30 days. Univariate and multivariate regression analyses were performed.</p><p><strong>Results: </strong>A total of 146 patients were diagnosed with new-onset HF: 68 with HFpEF and 78 with HFrEF. The patients with HFrEF were older than those with HFpEF (66.9 vs. 62 years, respectively, P = 0.008). Patients with HFrEF were more likely to have coronary artery disease, atrial fibrillation, or valvular heart disease than those with HFpEF (P < 0.05 for all). Patients with HFrEF rather than HFpEF were more likely to present with New York Heart Association class 3 - 4 dyspnea, orthopnea, paroxysmal nocturnal dyspnea or low cardiac output (P < 0.007 for all). Patients with HFpEF were more likely than those with HFpEF to have normal ECG at presentation (P < 0.001), and left bundle branch block (LBBB) was observed only in patients with HFrEF (P < 0.001). Resolution of symptoms within 30 days occurred in 75% of patients with HFpEF and 40% of patients with HFrEF (P < 0.001).</p><p><strong>Conclusions: </strong>Ambulatory patients with new-onset HFrEF were older, and had higher incidence of structural heart disease, in comparison to those with new-onset HFpEF. Patients presenting with HFrEF had more severe functional symptoms than those with HFpEF. Patients with HFpEF were more likely than those with HFpEF to have normal ECG at the time of presentation, and LBBB was strongly associated with HFrEF. Outpatients with HFrEF rather than HFpEF were less likely to respond to treatment.</p>\",\"PeriodicalId\":9424,\"journal\":{\"name\":\"Cardiology Research\",\"volume\":\"14 3\",\"pages\":\"201-210\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9f/82/cr-14-201.PMC10257507.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiology Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/cr1483\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/cr1483","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Differentiating Characteristics and Responses to Treatment of New-Onset Heart Failure With Preserved and Reduced Ejection Fraction in Ambulatory Patients.
Background: Differences in clinical presentation and therapy outcomes between heart failure with preserved ejection fraction (HFpEF) and heart failure with reduced ejection fraction (HFrEF) have been reported but described mainly among hospitalized patients. Because the population of outpatients with heart failure (HF) is increasing, we sought to discriminate the clinical presentation and responses to medical therapy in ambulatory patients with new-onset HFpEF vs. HFrEF.
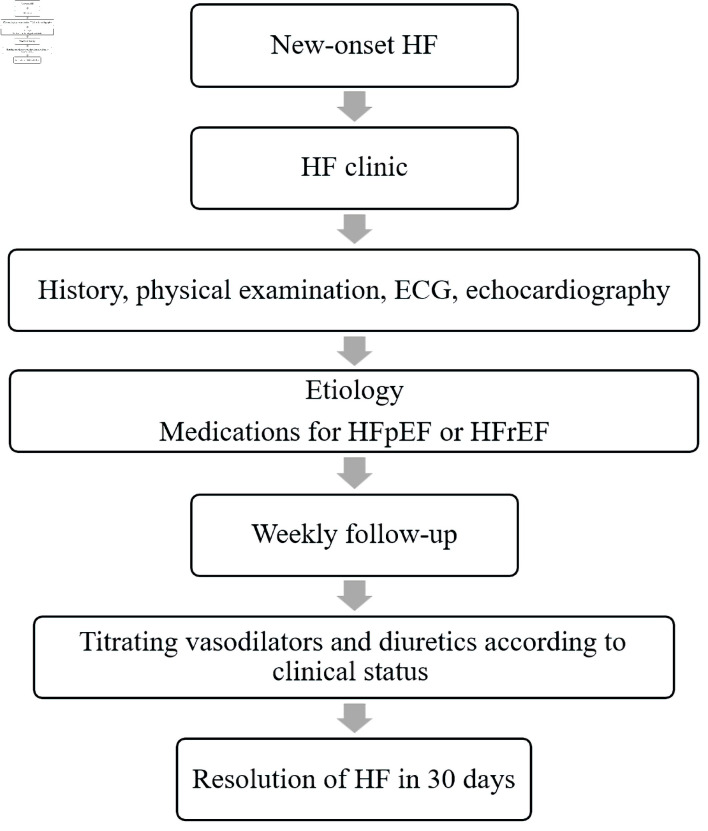
Methods: We retrospectively included all patients with new-onset HF treated at a single HF clinic in the past 4 years. Clinical data and electrocardiography (ECG) and echocardiography findings were recorded. Patients were followed up once weekly, and treatment response was evaluated according to symptoms resolution within 30 days. Univariate and multivariate regression analyses were performed.
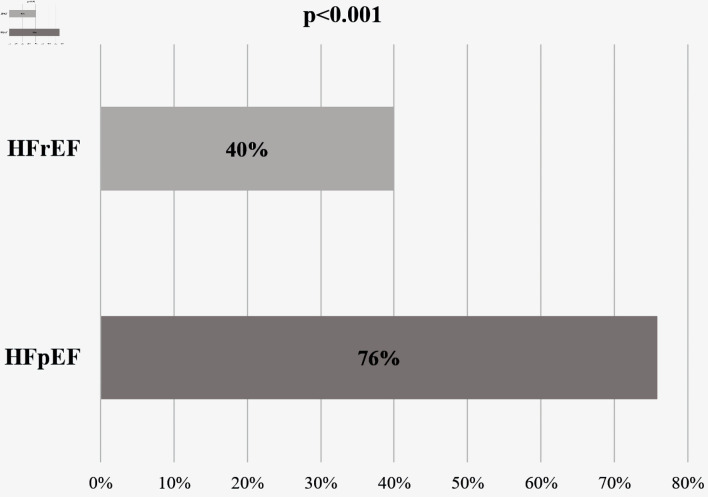
Results: A total of 146 patients were diagnosed with new-onset HF: 68 with HFpEF and 78 with HFrEF. The patients with HFrEF were older than those with HFpEF (66.9 vs. 62 years, respectively, P = 0.008). Patients with HFrEF were more likely to have coronary artery disease, atrial fibrillation, or valvular heart disease than those with HFpEF (P < 0.05 for all). Patients with HFrEF rather than HFpEF were more likely to present with New York Heart Association class 3 - 4 dyspnea, orthopnea, paroxysmal nocturnal dyspnea or low cardiac output (P < 0.007 for all). Patients with HFpEF were more likely than those with HFpEF to have normal ECG at presentation (P < 0.001), and left bundle branch block (LBBB) was observed only in patients with HFrEF (P < 0.001). Resolution of symptoms within 30 days occurred in 75% of patients with HFpEF and 40% of patients with HFrEF (P < 0.001).
Conclusions: Ambulatory patients with new-onset HFrEF were older, and had higher incidence of structural heart disease, in comparison to those with new-onset HFpEF. Patients presenting with HFrEF had more severe functional symptoms than those with HFpEF. Patients with HFpEF were more likely than those with HFpEF to have normal ECG at the time of presentation, and LBBB was strongly associated with HFrEF. Outpatients with HFrEF rather than HFpEF were less likely to respond to treatment.
期刊介绍:
Cardiology Research is an open access, peer-reviewed, international journal. All submissions relating to basic research and clinical practice of cardiology and cardiovascular medicine are in this journal''s scope. This journal focuses on publishing original research and observations in all cardiovascular medicine aspects. Manuscript types include original article, review, case report, short communication, book review, letter to the editor.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


