Sarju Ganatra, Sonu Abraham, Ashish Kumar, Rohan Parikh, Rushin Patel, Sumanth Khadke, Amudha Kumar, Victor Liu, Andrea Nathalie Rosas Diaz, Tomas G Neilan, David Martin, Bruce Hook, Sourbha S Dani, Aarti Asnani, Anju Nohria
{"title":"导管消融术治疗癌症患者心房颤动的有效性和安全性。","authors":"Sarju Ganatra, Sonu Abraham, Ashish Kumar, Rohan Parikh, Rushin Patel, Sumanth Khadke, Amudha Kumar, Victor Liu, Andrea Nathalie Rosas Diaz, Tomas G Neilan, David Martin, Bruce Hook, Sourbha S Dani, Aarti Asnani, Anju Nohria","doi":"10.1186/s40959-023-00171-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Though the incidence of atrial fibrillation (AF) is increased in patients with cancer, the effectiveness of catheter ablation (CA) for AF in patients with cancer is not well studied.</p><p><strong>Methods: </strong>We conducted a retrospective cohort study of patients who underwent CA for AF. Patients with a history of cancer within 5-years prior to, or those with an exposure to anthracyclines and/or thoracic radiation at any time prior to the index ablation were compared to patients without a history of cancer who underwent AF ablation. The primary outcome was freedom from AF [with or without anti-arrhythmic drugs (AADs), or need for repeat CA at 12-months post-ablation]. Secondary endpoints included freedom from AF at 12 months post-ablation with AADs and without AADs. Safety endpoints included bleeding, pulmonary vein stenosis, stroke, and cardiac tamponade. Multivariable regression analysis was performed to identify independent risk predictors of the primary outcome.</p><p><strong>Results: </strong>Among 502 patients included in the study, 251 (50%) had a history of cancer. Freedom from AF at 12 months did not differ between patients with and without cancer (83.3% vs 72.5%, p 0.28). The need for repeat ablation was also similar between groups (20.7% vs 27.5%, p 0.29). Multivariable regression analysis did not identify a history of cancer or cancer-related therapy as independent predictors of recurrent AF after ablation. There was no difference in safety endpoints between groups.</p><p><strong>Conclusion: </strong>CA is a safe and effective treatment for AF in patients with a history of cancer and those with exposure to potentially cardiotoxic therapy.</p>","PeriodicalId":72525,"journal":{"name":"","volume":"9 1","pages":"19"},"PeriodicalIF":0.0,"publicationDate":"2023-04-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10074889/pdf/","citationCount":"0","resultStr":"{\"title\":\"Efficacy and safety of catheter ablation for atrial fibrillation in patients with history of cancer.\",\"authors\":\"Sarju Ganatra, Sonu Abraham, Ashish Kumar, Rohan Parikh, Rushin Patel, Sumanth Khadke, Amudha Kumar, Victor Liu, Andrea Nathalie Rosas Diaz, Tomas G Neilan, David Martin, Bruce Hook, Sourbha S Dani, Aarti Asnani, Anju Nohria\",\"doi\":\"10.1186/s40959-023-00171-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Though the incidence of atrial fibrillation (AF) is increased in patients with cancer, the effectiveness of catheter ablation (CA) for AF in patients with cancer is not well studied.</p><p><strong>Methods: </strong>We conducted a retrospective cohort study of patients who underwent CA for AF. Patients with a history of cancer within 5-years prior to, or those with an exposure to anthracyclines and/or thoracic radiation at any time prior to the index ablation were compared to patients without a history of cancer who underwent AF ablation. The primary outcome was freedom from AF [with or without anti-arrhythmic drugs (AADs), or need for repeat CA at 12-months post-ablation]. Secondary endpoints included freedom from AF at 12 months post-ablation with AADs and without AADs. Safety endpoints included bleeding, pulmonary vein stenosis, stroke, and cardiac tamponade. Multivariable regression analysis was performed to identify independent risk predictors of the primary outcome.</p><p><strong>Results: </strong>Among 502 patients included in the study, 251 (50%) had a history of cancer. Freedom from AF at 12 months did not differ between patients with and without cancer (83.3% vs 72.5%, p 0.28). The need for repeat ablation was also similar between groups (20.7% vs 27.5%, p 0.29). Multivariable regression analysis did not identify a history of cancer or cancer-related therapy as independent predictors of recurrent AF after ablation. There was no difference in safety endpoints between groups.</p><p><strong>Conclusion: </strong>CA is a safe and effective treatment for AF in patients with a history of cancer and those with exposure to potentially cardiotoxic therapy.</p>\",\"PeriodicalId\":72525,\"journal\":{\"name\":\"\",\"volume\":\"9 1\",\"pages\":\"19\"},\"PeriodicalIF\":0.0,\"publicationDate\":\"2023-04-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10074889/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40959-023-00171-4\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-023-00171-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:虽然癌症患者心房颤动(AF)的发病率增加,但对癌症患者心房颤动导管消融术(CA)的疗效却没有很好的研究:我们对接受房颤导管消融术的患者进行了一项回顾性队列研究。我们将消融术前 5 年内有癌症病史或在消融术前任何时候接触过蒽环类药物和/或胸部放射线的患者与接受房颤消融术的无癌症病史患者进行了比较。主要结果是[使用或不使用抗心律失常药物 (AAD),或消融术后 12 个月时需要重复 CA]摆脱房颤。次要终点包括使用或不使用抗心律失常药物(AADs)消融术后 12 个月无房颤。安全性终点包括出血、肺静脉狭窄、中风和心脏填塞。研究人员进行了多变量回归分析,以确定主要结果的独立风险预测因素:在 502 名参与研究的患者中,251 人(50%)有癌症病史。有癌症和没有癌症的患者在12个月内免房颤的比例没有差异(83.3% vs 72.5%,P 0.28)。两组患者需要重复消融的比例也相似(20.7% vs 27.5%,P 0.29)。多变量回归分析并未发现癌症病史或癌症相关治疗是消融术后房颤复发的独立预测因素。各组间的安全性终点无差异:CA是一种安全有效的房颤治疗方法,适用于有癌症史和接受过潜在心脏毒性治疗的患者。
Efficacy and safety of catheter ablation for atrial fibrillation in patients with history of cancer.
Background: Though the incidence of atrial fibrillation (AF) is increased in patients with cancer, the effectiveness of catheter ablation (CA) for AF in patients with cancer is not well studied.
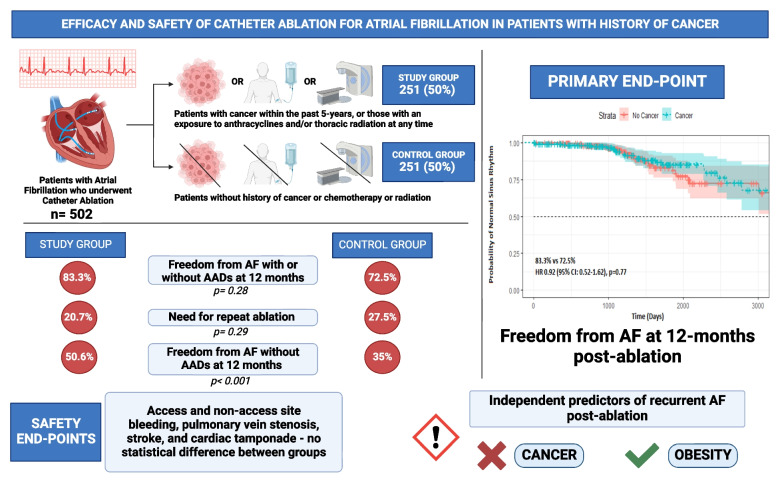
Methods: We conducted a retrospective cohort study of patients who underwent CA for AF. Patients with a history of cancer within 5-years prior to, or those with an exposure to anthracyclines and/or thoracic radiation at any time prior to the index ablation were compared to patients without a history of cancer who underwent AF ablation. The primary outcome was freedom from AF [with or without anti-arrhythmic drugs (AADs), or need for repeat CA at 12-months post-ablation]. Secondary endpoints included freedom from AF at 12 months post-ablation with AADs and without AADs. Safety endpoints included bleeding, pulmonary vein stenosis, stroke, and cardiac tamponade. Multivariable regression analysis was performed to identify independent risk predictors of the primary outcome.
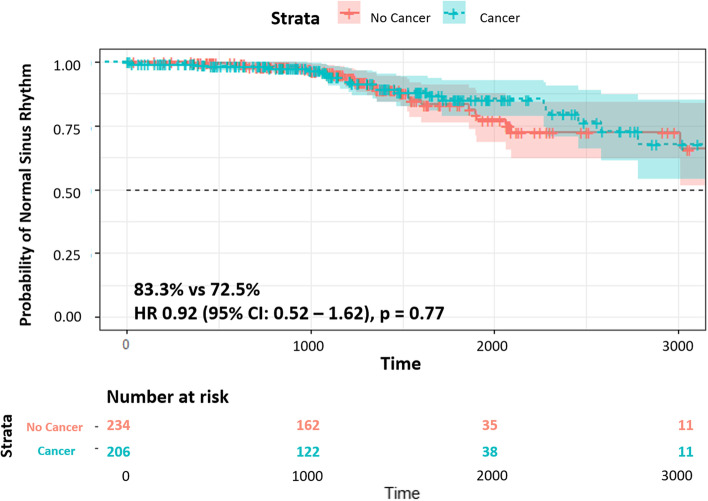
Results: Among 502 patients included in the study, 251 (50%) had a history of cancer. Freedom from AF at 12 months did not differ between patients with and without cancer (83.3% vs 72.5%, p 0.28). The need for repeat ablation was also similar between groups (20.7% vs 27.5%, p 0.29). Multivariable regression analysis did not identify a history of cancer or cancer-related therapy as independent predictors of recurrent AF after ablation. There was no difference in safety endpoints between groups.
Conclusion: CA is a safe and effective treatment for AF in patients with a history of cancer and those with exposure to potentially cardiotoxic therapy.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


