Alok Kumar, Ankur Joshi, Badal Parikh, Nikhil Tiwari, Ravi H Ramamurthy
{"title":"高频振荡通气治疗先天性心脏手术后呼吸衰竭的回顾性分析。","authors":"Alok Kumar, Ankur Joshi, Badal Parikh, Nikhil Tiwari, Ravi H Ramamurthy","doi":"10.5114/ait.2023.126219","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Pulmonary complications such as acute respiratory distress syndrome and refractory respiratory failure have been major causes of morbidity and mortality after cardiac surgery in children. Patients are usually transitioned to either high-frequency oscillatory ventilation (HFOV) or extracorporeal membrane oxygenation (ECMO) as \"salvage therapy\" when the maximal medical management and controlled mechanical ventilation (CMV) become ineffective.</p><p><strong>Material and methods: </strong>A retrospective review of paediatric patients who underwent congenital heart surgery and developed cardiorespiratory failure during their stay in a paediatric cardiac ICU, refractory to maximal CMV, was performed in the study. The outcomes assessed were respiratory variables such as SpO 2 , RR, oxygenation index (OI), P/F ratio, and ABG parameters in CMV and HFOV as predictors of survival.</p><p><strong>Results: </strong>Twenty-four children with cardiorespiratory failure were candidates for a transition to either HFOV ( n = 15) or VA ECMO ( n = 9) for refractory hypoxaemia; of these 24 patients, 13 (54.16%) survived. PaO2 showed a significant improvement in the survivors (P = 0.03). Improvement in the PaO 2 /FiO 2 (P/F ratio) after initiation of HFOV was associated with survival ( P < 0.001). pH, PaCO 2 , HCO 3 , FiO 2 , Paw, RR/Amp, SpO 2 , and OI also showed improvements in survivors but these were not statistically significant. The HFOV survivors had longer mechanical ventilation and ICU stay than non-survivors ( P = 0.13).</p><p><strong>Conclusions: </strong>HFOV was associated with improved gas exchange for paediatric patients who developed post-cardiac surgery refractory respiratory failure. HFOV can be considered as rescue therapy where ECMO has major financial implications.</p>","PeriodicalId":7750,"journal":{"name":"Anaesthesiology intensive therapy","volume":"55 1","pages":"60-67"},"PeriodicalIF":1.7000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/13/3f/AIT-55-50433.PMC10156544.pdf","citationCount":"0","resultStr":"{\"title\":\"High-frequency oscillatory ventilation for respiratory failure after congenital heart surgery: a retrospective analysis.\",\"authors\":\"Alok Kumar, Ankur Joshi, Badal Parikh, Nikhil Tiwari, Ravi H Ramamurthy\",\"doi\":\"10.5114/ait.2023.126219\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Pulmonary complications such as acute respiratory distress syndrome and refractory respiratory failure have been major causes of morbidity and mortality after cardiac surgery in children. Patients are usually transitioned to either high-frequency oscillatory ventilation (HFOV) or extracorporeal membrane oxygenation (ECMO) as \\\"salvage therapy\\\" when the maximal medical management and controlled mechanical ventilation (CMV) become ineffective.</p><p><strong>Material and methods: </strong>A retrospective review of paediatric patients who underwent congenital heart surgery and developed cardiorespiratory failure during their stay in a paediatric cardiac ICU, refractory to maximal CMV, was performed in the study. The outcomes assessed were respiratory variables such as SpO 2 , RR, oxygenation index (OI), P/F ratio, and ABG parameters in CMV and HFOV as predictors of survival.</p><p><strong>Results: </strong>Twenty-four children with cardiorespiratory failure were candidates for a transition to either HFOV ( n = 15) or VA ECMO ( n = 9) for refractory hypoxaemia; of these 24 patients, 13 (54.16%) survived. PaO2 showed a significant improvement in the survivors (P = 0.03). Improvement in the PaO 2 /FiO 2 (P/F ratio) after initiation of HFOV was associated with survival ( P < 0.001). pH, PaCO 2 , HCO 3 , FiO 2 , Paw, RR/Amp, SpO 2 , and OI also showed improvements in survivors but these were not statistically significant. The HFOV survivors had longer mechanical ventilation and ICU stay than non-survivors ( P = 0.13).</p><p><strong>Conclusions: </strong>HFOV was associated with improved gas exchange for paediatric patients who developed post-cardiac surgery refractory respiratory failure. HFOV can be considered as rescue therapy where ECMO has major financial implications.</p>\",\"PeriodicalId\":7750,\"journal\":{\"name\":\"Anaesthesiology intensive therapy\",\"volume\":\"55 1\",\"pages\":\"60-67\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/13/3f/AIT-55-50433.PMC10156544.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Anaesthesiology intensive therapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5114/ait.2023.126219\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anaesthesiology intensive therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/ait.2023.126219","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
High-frequency oscillatory ventilation for respiratory failure after congenital heart surgery: a retrospective analysis.
Introduction: Pulmonary complications such as acute respiratory distress syndrome and refractory respiratory failure have been major causes of morbidity and mortality after cardiac surgery in children. Patients are usually transitioned to either high-frequency oscillatory ventilation (HFOV) or extracorporeal membrane oxygenation (ECMO) as "salvage therapy" when the maximal medical management and controlled mechanical ventilation (CMV) become ineffective.
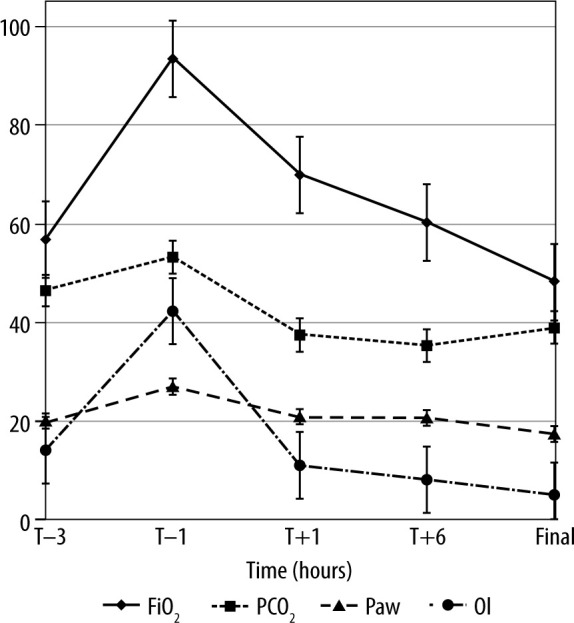
Material and methods: A retrospective review of paediatric patients who underwent congenital heart surgery and developed cardiorespiratory failure during their stay in a paediatric cardiac ICU, refractory to maximal CMV, was performed in the study. The outcomes assessed were respiratory variables such as SpO 2 , RR, oxygenation index (OI), P/F ratio, and ABG parameters in CMV and HFOV as predictors of survival.
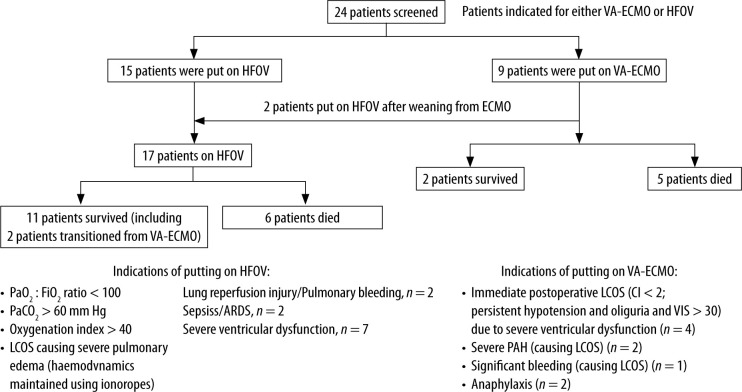
Results: Twenty-four children with cardiorespiratory failure were candidates for a transition to either HFOV ( n = 15) or VA ECMO ( n = 9) for refractory hypoxaemia; of these 24 patients, 13 (54.16%) survived. PaO2 showed a significant improvement in the survivors (P = 0.03). Improvement in the PaO 2 /FiO 2 (P/F ratio) after initiation of HFOV was associated with survival ( P < 0.001). pH, PaCO 2 , HCO 3 , FiO 2 , Paw, RR/Amp, SpO 2 , and OI also showed improvements in survivors but these were not statistically significant. The HFOV survivors had longer mechanical ventilation and ICU stay than non-survivors ( P = 0.13).
Conclusions: HFOV was associated with improved gas exchange for paediatric patients who developed post-cardiac surgery refractory respiratory failure. HFOV can be considered as rescue therapy where ECMO has major financial implications.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


