Natasha L Orr, Arianne Albert, Yang Doris Liu, Amy Lum, JooYoon Hong, Catalina L Ionescu, Janine Senz, Tayyebeh M Nazeran, Anna F Lee, Heather Noga, Kate Lawrenson, Catherine Allaire, Christina Williams, Mohamed A Bedaiwy, Michael S Anglesio, Paul J Yong
{"title":"KRAS突变与子宫内膜异位症的疾病负担","authors":"Natasha L Orr, Arianne Albert, Yang Doris Liu, Amy Lum, JooYoon Hong, Catalina L Ionescu, Janine Senz, Tayyebeh M Nazeran, Anna F Lee, Heather Noga, Kate Lawrenson, Catherine Allaire, Christina Williams, Mohamed A Bedaiwy, Michael S Anglesio, Paul J Yong","doi":"10.1002/cjp2.317","DOIUrl":null,"url":null,"abstract":"<p>The clinical phenotype of somatic mutations in endometriosis is unknown. The objective was to determine whether somatic <i>KRAS</i> mutations were associated with greater disease burden in endometriosis (i.e. more severe subtypes and higher stage). This prospective longitudinal cohort study included 122 subjects undergoing endometriosis surgery at a tertiary referral center between 2013 and 2017, with 5–9 years of follow-up. Somatic activating <i>KRAS</i> codon 12 mutations were detected in endometriosis lesions using droplet digital PCR. <i>KRAS</i> mutation status for each subject was coded as present (<i>KRAS</i> mutation in at least one endometriosis sample in a subject) or absent. Standardized clinical phenotyping for each subject was carried out via linkage to a prospective registry. Primary outcome was anatomic disease burden, based on distribution of subtypes (deep infiltrating endometriosis, ovarian endometrioma, and superficial peritoneal endometriosis) and surgical staging (Stages I–IV). Secondary outcomes were markers of surgical difficulty, demographics, pain scores, and risk of re-operation. <i>KRAS</i> mutation presence was higher in subjects with deep infiltrating endometriosis or endometrioma lesions only (57.9%; 11/19) and subjects with mixed subtypes (60.6%; 40/66), compared with those with superficial endometriosis only (35.1%; 13/37) (<i>p</i> = 0.04). <i>KRAS</i> mutation was present in 27.6% (8/29) of Stage I cases, in comparison to 65.0% (13/20) of Stage II, 63.0% (17/27) of Stage III, and 58.1% (25/43) of Stage IV cases (<i>p</i> = 0.02). <i>KRAS</i> mutation was also associated with greater surgical difficulty (ureterolysis) (relative risk [RR] = 1.47, 95% CI: 1.02–2.11) and non-Caucasian ethnicity (RR = 0.64, 95% CI: 0.47–0.89). Pain severities did not differ based on <i>KRAS</i> mutation status, at either baseline or follow-up. Re-operation rates were low overall, occurring in 17.2% with <i>KRAS</i> mutation compared with 10.3% without (RR = 1.66, 95% CI: 0.66–4.21). In conclusion, <i>KRAS</i> mutations were associated with greater anatomic severity of endometriosis, resulting in increased surgical difficulty. Somatic cancer-driver mutations may inform a future molecular classification of endometriosis.</p>","PeriodicalId":48612,"journal":{"name":"Journal of Pathology Clinical Research","volume":"9 4","pages":"302-312"},"PeriodicalIF":3.4000,"publicationDate":"2023-03-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://pathsocjournals.onlinelibrary.wiley.com/doi/epdf/10.1002/cjp2.317","citationCount":"1","resultStr":"{\"title\":\"KRAS mutations and endometriosis burden of disease\",\"authors\":\"Natasha L Orr, Arianne Albert, Yang Doris Liu, Amy Lum, JooYoon Hong, Catalina L Ionescu, Janine Senz, Tayyebeh M Nazeran, Anna F Lee, Heather Noga, Kate Lawrenson, Catherine Allaire, Christina Williams, Mohamed A Bedaiwy, Michael S Anglesio, Paul J Yong\",\"doi\":\"10.1002/cjp2.317\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The clinical phenotype of somatic mutations in endometriosis is unknown. The objective was to determine whether somatic <i>KRAS</i> mutations were associated with greater disease burden in endometriosis (i.e. more severe subtypes and higher stage). This prospective longitudinal cohort study included 122 subjects undergoing endometriosis surgery at a tertiary referral center between 2013 and 2017, with 5–9 years of follow-up. Somatic activating <i>KRAS</i> codon 12 mutations were detected in endometriosis lesions using droplet digital PCR. <i>KRAS</i> mutation status for each subject was coded as present (<i>KRAS</i> mutation in at least one endometriosis sample in a subject) or absent. Standardized clinical phenotyping for each subject was carried out via linkage to a prospective registry. Primary outcome was anatomic disease burden, based on distribution of subtypes (deep infiltrating endometriosis, ovarian endometrioma, and superficial peritoneal endometriosis) and surgical staging (Stages I–IV). Secondary outcomes were markers of surgical difficulty, demographics, pain scores, and risk of re-operation. <i>KRAS</i> mutation presence was higher in subjects with deep infiltrating endometriosis or endometrioma lesions only (57.9%; 11/19) and subjects with mixed subtypes (60.6%; 40/66), compared with those with superficial endometriosis only (35.1%; 13/37) (<i>p</i> = 0.04). <i>KRAS</i> mutation was present in 27.6% (8/29) of Stage I cases, in comparison to 65.0% (13/20) of Stage II, 63.0% (17/27) of Stage III, and 58.1% (25/43) of Stage IV cases (<i>p</i> = 0.02). <i>KRAS</i> mutation was also associated with greater surgical difficulty (ureterolysis) (relative risk [RR] = 1.47, 95% CI: 1.02–2.11) and non-Caucasian ethnicity (RR = 0.64, 95% CI: 0.47–0.89). Pain severities did not differ based on <i>KRAS</i> mutation status, at either baseline or follow-up. Re-operation rates were low overall, occurring in 17.2% with <i>KRAS</i> mutation compared with 10.3% without (RR = 1.66, 95% CI: 0.66–4.21). In conclusion, <i>KRAS</i> mutations were associated with greater anatomic severity of endometriosis, resulting in increased surgical difficulty. Somatic cancer-driver mutations may inform a future molecular classification of endometriosis.</p>\",\"PeriodicalId\":48612,\"journal\":{\"name\":\"Journal of Pathology Clinical Research\",\"volume\":\"9 4\",\"pages\":\"302-312\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2023-03-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://pathsocjournals.onlinelibrary.wiley.com/doi/epdf/10.1002/cjp2.317\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Pathology Clinical Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cjp2.317\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PATHOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Pathology Clinical Research","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cjp2.317","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PATHOLOGY","Score":null,"Total":0}
KRAS mutations and endometriosis burden of disease
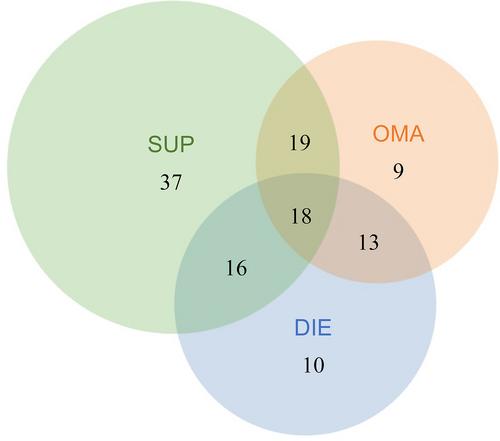
The clinical phenotype of somatic mutations in endometriosis is unknown. The objective was to determine whether somatic KRAS mutations were associated with greater disease burden in endometriosis (i.e. more severe subtypes and higher stage). This prospective longitudinal cohort study included 122 subjects undergoing endometriosis surgery at a tertiary referral center between 2013 and 2017, with 5–9 years of follow-up. Somatic activating KRAS codon 12 mutations were detected in endometriosis lesions using droplet digital PCR. KRAS mutation status for each subject was coded as present (KRAS mutation in at least one endometriosis sample in a subject) or absent. Standardized clinical phenotyping for each subject was carried out via linkage to a prospective registry. Primary outcome was anatomic disease burden, based on distribution of subtypes (deep infiltrating endometriosis, ovarian endometrioma, and superficial peritoneal endometriosis) and surgical staging (Stages I–IV). Secondary outcomes were markers of surgical difficulty, demographics, pain scores, and risk of re-operation. KRAS mutation presence was higher in subjects with deep infiltrating endometriosis or endometrioma lesions only (57.9%; 11/19) and subjects with mixed subtypes (60.6%; 40/66), compared with those with superficial endometriosis only (35.1%; 13/37) (p = 0.04). KRAS mutation was present in 27.6% (8/29) of Stage I cases, in comparison to 65.0% (13/20) of Stage II, 63.0% (17/27) of Stage III, and 58.1% (25/43) of Stage IV cases (p = 0.02). KRAS mutation was also associated with greater surgical difficulty (ureterolysis) (relative risk [RR] = 1.47, 95% CI: 1.02–2.11) and non-Caucasian ethnicity (RR = 0.64, 95% CI: 0.47–0.89). Pain severities did not differ based on KRAS mutation status, at either baseline or follow-up. Re-operation rates were low overall, occurring in 17.2% with KRAS mutation compared with 10.3% without (RR = 1.66, 95% CI: 0.66–4.21). In conclusion, KRAS mutations were associated with greater anatomic severity of endometriosis, resulting in increased surgical difficulty. Somatic cancer-driver mutations may inform a future molecular classification of endometriosis.
期刊介绍:
The Journal of Pathology: Clinical Research and The Journal of Pathology serve as translational bridges between basic biomedical science and clinical medicine with particular emphasis on, but not restricted to, tissue based studies.
The focus of The Journal of Pathology: Clinical Research is the publication of studies that illuminate the clinical relevance of research in the broad area of the study of disease. Appropriately powered and validated studies with novel diagnostic, prognostic and predictive significance, and biomarker discover and validation, will be welcomed. Studies with a predominantly mechanistic basis will be more appropriate for the companion Journal of Pathology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


