Varshitha Tumkur Panduranga, Asher Gorantla, Asad Ahmed, Jacob Sabu, Mary Mallappallil, Sabu John
{"title":"一例罕见的充血性心力衰竭由于孤立主动脉瓣疾病继发于风湿热的中年男子。","authors":"Varshitha Tumkur Panduranga, Asher Gorantla, Asad Ahmed, Jacob Sabu, Mary Mallappallil, Sabu John","doi":"10.14740/jmc4090","DOIUrl":null,"url":null,"abstract":"<p><p>Rheumatic heart disease (RHD) is commonly seen in people from developing and low-income countries. More cases are being recorded in developed countries due to migration and globalization. RHD develops in people with a history of rheumatic fever; it is an autoimmune response to group A streptococcal infection due to similarities at the molecular level. Congestive heart failure, arrhythmia, atrial fibrillation, stroke, and infective endocarditis are a few of the many complications associated with RHD. Here we present a case of a 48-year-old male with a past medical history of rheumatic fever at the age of 12 years, who presented to the emergency room (ER) complaining of bilateral ankle swelling, dyspnea on exertion, and palpitations. The patient was tachycardic with a heart rate of 146 beats per minute and tachypneic with a respiratory rate of 22 breaths per minute. On physical exam, there was a harsh systolic and diastolic murmur at the right upper sternal border. A 12-lead electrocardiogram (EKG) revealed atrial flutter with a variable block. Chest X-ray revealed an enlarged cardiac silhouette with a pro-brain natriuretic peptide (proBNP) of 2,772 pg/mL (normal ≤ 125 pg/mL). The patient was stabilized with metoprolol and furosemide and was admitted to the hospital for further investigation. Transthoracic echocardiogram showed left ventricular ejection fraction (LVEF) of 50-55% with severe concentric hypertrophy of the left ventricle with a severely dilated left atrium. Increased thickness of the aortic valve with severe stenosis and a peak gradient of 139 mm Hg and a mean gradient of 82 mm Hg was noted. The valve area was measured to be 0.8 cm<sup>2</sup>. Transesophageal echocardiogram showed a tri-leaflet aortic valve with commissural fusion of valve cusps with severe leaflet thickening consistent with rheumatic valve disease. The patient underwent tissue aortic valve replacement with a bioprosthetic valve. The pathology report showed extensive fibrosis and calcification of the aortic valve. The patient came in for a follow-up visit 6 months later and expressed feeling better and more active.</p>","PeriodicalId":16279,"journal":{"name":"Journal of Medical Cases","volume":"14 5","pages":"149-154"},"PeriodicalIF":0.0000,"publicationDate":"2023-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0f/06/jmc-14-149.PMC10251705.pdf","citationCount":"0","resultStr":"{\"title\":\"A Rare Case of Congestive Heart Failure due to Isolated Aortic Valve Disease in a Middle-Aged Man Secondary to Rheumatic Fever.\",\"authors\":\"Varshitha Tumkur Panduranga, Asher Gorantla, Asad Ahmed, Jacob Sabu, Mary Mallappallil, Sabu John\",\"doi\":\"10.14740/jmc4090\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Rheumatic heart disease (RHD) is commonly seen in people from developing and low-income countries. More cases are being recorded in developed countries due to migration and globalization. RHD develops in people with a history of rheumatic fever; it is an autoimmune response to group A streptococcal infection due to similarities at the molecular level. Congestive heart failure, arrhythmia, atrial fibrillation, stroke, and infective endocarditis are a few of the many complications associated with RHD. Here we present a case of a 48-year-old male with a past medical history of rheumatic fever at the age of 12 years, who presented to the emergency room (ER) complaining of bilateral ankle swelling, dyspnea on exertion, and palpitations. The patient was tachycardic with a heart rate of 146 beats per minute and tachypneic with a respiratory rate of 22 breaths per minute. On physical exam, there was a harsh systolic and diastolic murmur at the right upper sternal border. A 12-lead electrocardiogram (EKG) revealed atrial flutter with a variable block. Chest X-ray revealed an enlarged cardiac silhouette with a pro-brain natriuretic peptide (proBNP) of 2,772 pg/mL (normal ≤ 125 pg/mL). The patient was stabilized with metoprolol and furosemide and was admitted to the hospital for further investigation. Transthoracic echocardiogram showed left ventricular ejection fraction (LVEF) of 50-55% with severe concentric hypertrophy of the left ventricle with a severely dilated left atrium. Increased thickness of the aortic valve with severe stenosis and a peak gradient of 139 mm Hg and a mean gradient of 82 mm Hg was noted. The valve area was measured to be 0.8 cm<sup>2</sup>. Transesophageal echocardiogram showed a tri-leaflet aortic valve with commissural fusion of valve cusps with severe leaflet thickening consistent with rheumatic valve disease. The patient underwent tissue aortic valve replacement with a bioprosthetic valve. The pathology report showed extensive fibrosis and calcification of the aortic valve. The patient came in for a follow-up visit 6 months later and expressed feeling better and more active.</p>\",\"PeriodicalId\":16279,\"journal\":{\"name\":\"Journal of Medical Cases\",\"volume\":\"14 5\",\"pages\":\"149-154\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0f/06/jmc-14-149.PMC10251705.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Medical Cases\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/jmc4090\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Medical Cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jmc4090","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
A Rare Case of Congestive Heart Failure due to Isolated Aortic Valve Disease in a Middle-Aged Man Secondary to Rheumatic Fever.
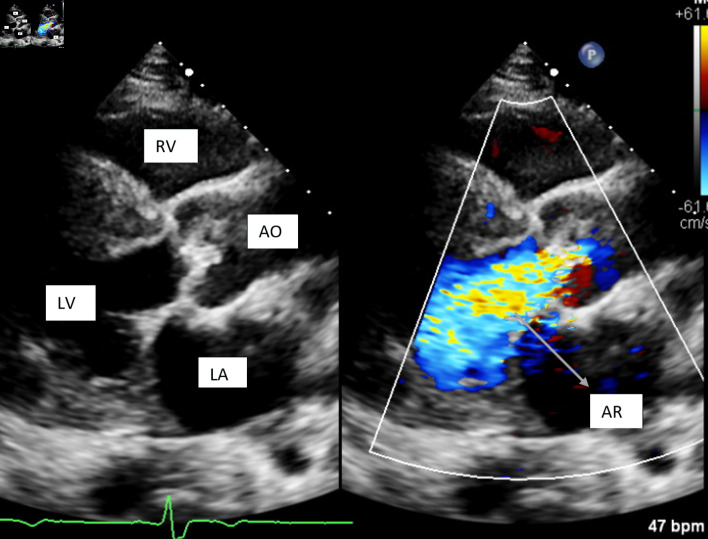
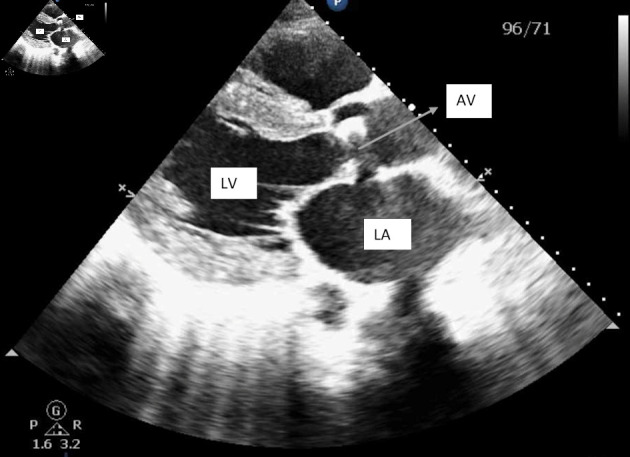
Rheumatic heart disease (RHD) is commonly seen in people from developing and low-income countries. More cases are being recorded in developed countries due to migration and globalization. RHD develops in people with a history of rheumatic fever; it is an autoimmune response to group A streptococcal infection due to similarities at the molecular level. Congestive heart failure, arrhythmia, atrial fibrillation, stroke, and infective endocarditis are a few of the many complications associated with RHD. Here we present a case of a 48-year-old male with a past medical history of rheumatic fever at the age of 12 years, who presented to the emergency room (ER) complaining of bilateral ankle swelling, dyspnea on exertion, and palpitations. The patient was tachycardic with a heart rate of 146 beats per minute and tachypneic with a respiratory rate of 22 breaths per minute. On physical exam, there was a harsh systolic and diastolic murmur at the right upper sternal border. A 12-lead electrocardiogram (EKG) revealed atrial flutter with a variable block. Chest X-ray revealed an enlarged cardiac silhouette with a pro-brain natriuretic peptide (proBNP) of 2,772 pg/mL (normal ≤ 125 pg/mL). The patient was stabilized with metoprolol and furosemide and was admitted to the hospital for further investigation. Transthoracic echocardiogram showed left ventricular ejection fraction (LVEF) of 50-55% with severe concentric hypertrophy of the left ventricle with a severely dilated left atrium. Increased thickness of the aortic valve with severe stenosis and a peak gradient of 139 mm Hg and a mean gradient of 82 mm Hg was noted. The valve area was measured to be 0.8 cm2. Transesophageal echocardiogram showed a tri-leaflet aortic valve with commissural fusion of valve cusps with severe leaflet thickening consistent with rheumatic valve disease. The patient underwent tissue aortic valve replacement with a bioprosthetic valve. The pathology report showed extensive fibrosis and calcification of the aortic valve. The patient came in for a follow-up visit 6 months later and expressed feeling better and more active.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


