Christopher Traenka, Johannes Lorscheider, Christian Hametner, Philipp Baumgartner, Jan Gralla, Mauro Magoni, Nicolas Martinez-Majander, Barbara Casolla, Katharina Feil, Rosario Pascarella, Panagiotis Papanagiotou, Annika Nordanstig, Visnja Padjen, Carlo W Cereda, Marios Psychogios, Christian H Nolte, Andrea Zini, Patrik Michel, Yannick Béjot, Andreas Kastrup, Marialuisa Zedde, Georg Kägi, Lars Kellert, Hilde Henon, Sami Curtze, Alessandro Pezzini, Marcel Arnold, Susanne Wegener, Peter Ringleb, Turgut Tatlisumak, Paul J Nederkoorn, Stefan T Engelter, Henrik Gensicke
{"title":"颈动脉夹层所致大血管闭塞的再通治疗:EVA-TRISP合作的队列研究。","authors":"Christopher Traenka, Johannes Lorscheider, Christian Hametner, Philipp Baumgartner, Jan Gralla, Mauro Magoni, Nicolas Martinez-Majander, Barbara Casolla, Katharina Feil, Rosario Pascarella, Panagiotis Papanagiotou, Annika Nordanstig, Visnja Padjen, Carlo W Cereda, Marios Psychogios, Christian H Nolte, Andrea Zini, Patrik Michel, Yannick Béjot, Andreas Kastrup, Marialuisa Zedde, Georg Kägi, Lars Kellert, Hilde Henon, Sami Curtze, Alessandro Pezzini, Marcel Arnold, Susanne Wegener, Peter Ringleb, Turgut Tatlisumak, Paul J Nederkoorn, Stefan T Engelter, Henrik Gensicke","doi":"10.5853/jos.2022.03370","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>This study aimed to investigate the effect of endovascular treatment (EVT, with or without intravenous thrombolysis [IVT]) versus IVT alone on outcomes in patients with acute ischemic stroke (AIS) and intracranial large vessel occlusion (LVO) attributable to cervical artery dissection (CeAD).</p><p><strong>Methods: </strong>This multinational cohort study was conducted based on prospectively collected data from the EVA-TRISP (EndoVAscular treatment and ThRombolysis for Ischemic Stroke Patients) collaboration. Consecutive patients (2015-2019) with AIS-LVO attributable to CeAD treated with EVT and/or IVT were included. Primary outcome measures were (1) favorable 3-month outcome (modified Rankin Scale score 0-2) and (2) complete recanalization (thrombolysis in cerebral infarction scale 2b/3). Odds ratios with 95% confidence intervals (OR [95% CI]) from logistic regression models were calculated (unadjusted, adjusted). Secondary analyses were performed in the patients with LVO in the anterior circulation (LVOant) including propensity score matching.</p><p><strong>Results: </strong>Among 290 patients, 222 (76.6%) had EVT and 68 (23.4%) IVT alone. EVT-treated patients had more severe strokes (National Institutes of Health Stroke Scale score, median [interquartile range]: 14 [10-19] vs. 4 [2-7], P<0.001). The frequency of favorable 3-month outcome did not differ significantly between both groups (EVT: 64.0% vs. IVT: 86.8%; ORadjusted 0.56 [0.24-1.32]). EVT was associated with higher rates of recanalization (80.5% vs. 40.7%; ORadjusted 8.85 [4.28-18.29]) compared to IVT. All secondary analyses showed higher recanalization rates in the EVT-group, which however never translated into better functional outcome rates compared to the IVT-group.</p><p><strong>Conclusion: </strong>We observed no signal of superiority of EVT over IVT regarding functional outcome in CeAD-patients with AIS and LVO despite higher rates of complete recanalization with EVT. Whether pathophysiological CeAD-characteristics or their younger age might explain this observation deserves further research.</p>","PeriodicalId":17135,"journal":{"name":"Journal of Stroke","volume":"25 2","pages":"272-281"},"PeriodicalIF":8.6000,"publicationDate":"2023-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6f/56/jos-2022-03370.PMC10250869.pdf","citationCount":"0","resultStr":"{\"title\":\"Recanalization Therapies for Large Vessel Occlusion Due to Cervical Artery Dissection: A Cohort Study of the EVA-TRISP Collaboration.\",\"authors\":\"Christopher Traenka, Johannes Lorscheider, Christian Hametner, Philipp Baumgartner, Jan Gralla, Mauro Magoni, Nicolas Martinez-Majander, Barbara Casolla, Katharina Feil, Rosario Pascarella, Panagiotis Papanagiotou, Annika Nordanstig, Visnja Padjen, Carlo W Cereda, Marios Psychogios, Christian H Nolte, Andrea Zini, Patrik Michel, Yannick Béjot, Andreas Kastrup, Marialuisa Zedde, Georg Kägi, Lars Kellert, Hilde Henon, Sami Curtze, Alessandro Pezzini, Marcel Arnold, Susanne Wegener, Peter Ringleb, Turgut Tatlisumak, Paul J Nederkoorn, Stefan T Engelter, Henrik Gensicke\",\"doi\":\"10.5853/jos.2022.03370\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and purpose: </strong>This study aimed to investigate the effect of endovascular treatment (EVT, with or without intravenous thrombolysis [IVT]) versus IVT alone on outcomes in patients with acute ischemic stroke (AIS) and intracranial large vessel occlusion (LVO) attributable to cervical artery dissection (CeAD).</p><p><strong>Methods: </strong>This multinational cohort study was conducted based on prospectively collected data from the EVA-TRISP (EndoVAscular treatment and ThRombolysis for Ischemic Stroke Patients) collaboration. Consecutive patients (2015-2019) with AIS-LVO attributable to CeAD treated with EVT and/or IVT were included. Primary outcome measures were (1) favorable 3-month outcome (modified Rankin Scale score 0-2) and (2) complete recanalization (thrombolysis in cerebral infarction scale 2b/3). Odds ratios with 95% confidence intervals (OR [95% CI]) from logistic regression models were calculated (unadjusted, adjusted). Secondary analyses were performed in the patients with LVO in the anterior circulation (LVOant) including propensity score matching.</p><p><strong>Results: </strong>Among 290 patients, 222 (76.6%) had EVT and 68 (23.4%) IVT alone. EVT-treated patients had more severe strokes (National Institutes of Health Stroke Scale score, median [interquartile range]: 14 [10-19] vs. 4 [2-7], P<0.001). The frequency of favorable 3-month outcome did not differ significantly between both groups (EVT: 64.0% vs. IVT: 86.8%; ORadjusted 0.56 [0.24-1.32]). EVT was associated with higher rates of recanalization (80.5% vs. 40.7%; ORadjusted 8.85 [4.28-18.29]) compared to IVT. All secondary analyses showed higher recanalization rates in the EVT-group, which however never translated into better functional outcome rates compared to the IVT-group.</p><p><strong>Conclusion: </strong>We observed no signal of superiority of EVT over IVT regarding functional outcome in CeAD-patients with AIS and LVO despite higher rates of complete recanalization with EVT. Whether pathophysiological CeAD-characteristics or their younger age might explain this observation deserves further research.</p>\",\"PeriodicalId\":17135,\"journal\":{\"name\":\"Journal of Stroke\",\"volume\":\"25 2\",\"pages\":\"272-281\"},\"PeriodicalIF\":8.6000,\"publicationDate\":\"2023-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6f/56/jos-2022-03370.PMC10250869.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Stroke\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5853/jos.2022.03370\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Stroke","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5853/jos.2022.03370","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Recanalization Therapies for Large Vessel Occlusion Due to Cervical Artery Dissection: A Cohort Study of the EVA-TRISP Collaboration.
Background and purpose: This study aimed to investigate the effect of endovascular treatment (EVT, with or without intravenous thrombolysis [IVT]) versus IVT alone on outcomes in patients with acute ischemic stroke (AIS) and intracranial large vessel occlusion (LVO) attributable to cervical artery dissection (CeAD).
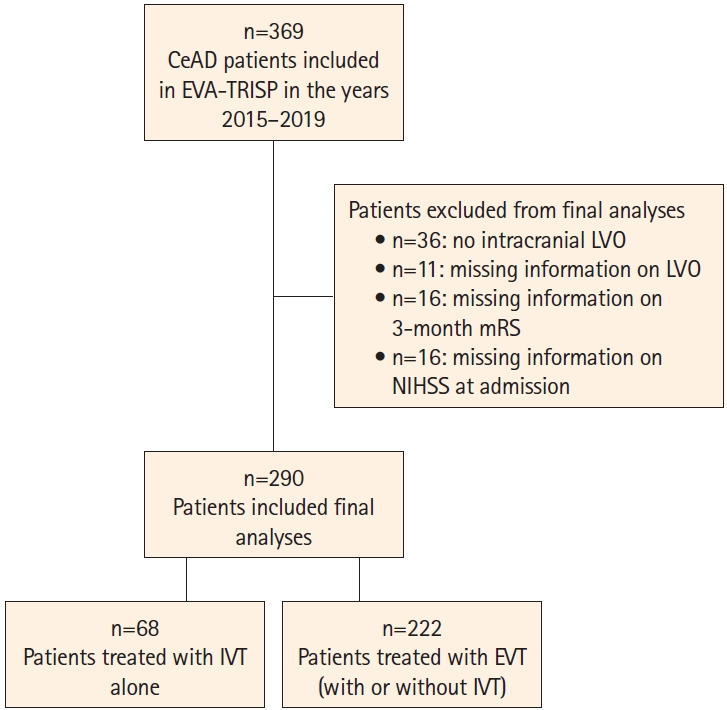
Methods: This multinational cohort study was conducted based on prospectively collected data from the EVA-TRISP (EndoVAscular treatment and ThRombolysis for Ischemic Stroke Patients) collaboration. Consecutive patients (2015-2019) with AIS-LVO attributable to CeAD treated with EVT and/or IVT were included. Primary outcome measures were (1) favorable 3-month outcome (modified Rankin Scale score 0-2) and (2) complete recanalization (thrombolysis in cerebral infarction scale 2b/3). Odds ratios with 95% confidence intervals (OR [95% CI]) from logistic regression models were calculated (unadjusted, adjusted). Secondary analyses were performed in the patients with LVO in the anterior circulation (LVOant) including propensity score matching.
Results: Among 290 patients, 222 (76.6%) had EVT and 68 (23.4%) IVT alone. EVT-treated patients had more severe strokes (National Institutes of Health Stroke Scale score, median [interquartile range]: 14 [10-19] vs. 4 [2-7], P<0.001). The frequency of favorable 3-month outcome did not differ significantly between both groups (EVT: 64.0% vs. IVT: 86.8%; ORadjusted 0.56 [0.24-1.32]). EVT was associated with higher rates of recanalization (80.5% vs. 40.7%; ORadjusted 8.85 [4.28-18.29]) compared to IVT. All secondary analyses showed higher recanalization rates in the EVT-group, which however never translated into better functional outcome rates compared to the IVT-group.
Conclusion: We observed no signal of superiority of EVT over IVT regarding functional outcome in CeAD-patients with AIS and LVO despite higher rates of complete recanalization with EVT. Whether pathophysiological CeAD-characteristics or their younger age might explain this observation deserves further research.
Journal of StrokeCLINICAL NEUROLOGYPERIPHERAL VASCULAR DISE-PERIPHERAL VASCULAR DISEASE
CiteScore
11.00
自引率
3.70%
发文量
52
审稿时长
12 weeks
期刊介绍:
The Journal of Stroke (JoS) is a peer-reviewed publication that focuses on clinical and basic investigation of cerebral circulation and associated diseases in stroke-related fields. Its aim is to enhance patient management, education, clinical or experimental research, and professionalism. The journal covers various areas of stroke research, including pathophysiology, risk factors, symptomatology, imaging, treatment, and rehabilitation. Basic science research is included when it provides clinically relevant information. The JoS is particularly interested in studies that highlight characteristics of stroke in the Asian population, as they are underrepresented in the literature.
The JoS had an impact factor of 8.2 in 2022 and aims to provide high-quality research papers to readers while maintaining a strong reputation. It is published three times a year, on the last day of January, May, and September. The online version of the journal is considered the main version as it includes all available content. Supplementary issues are occasionally published.
The journal is indexed in various databases, including SCI(E), Pubmed, PubMed Central, Scopus, KoreaMed, Komci, Synapse, Science Central, Google Scholar, and DOI/Crossref. It is also the official journal of the Korean Stroke Society since 1999, with the abbreviated title J Stroke.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


