{"title":"股骨内翻胫骨外翻截骨术(FVTVO)治疗伴有严重关节线倾斜的中性膝关节骨性关节炎,使其能够恢复体育活动:一个病例系列研究","authors":"Ryuichi Nakamura , Masaki Amemiya , Tomoyuki Shimakawa , Masaki Takahashi , Kazunari Kuroda , Yasuo Katsuki , Akira Okano","doi":"10.1016/j.asmart.2023.01.002","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Re-alignment surgeries for uni-compartmental knee osteoarthritis, such as high tibial osteotomy (HTO) for varus knees or distal femoral osteotomy (DFO) for valgus knees, are recognized as standard strategies. However, the treatment strategy has not been established for patients with a neutrally-aligned osteoarthritic knee with severe joint line obliquity (JLO) owing to the combination of a valgus femur and a varus tibia; i.e., type II coronal plane alignment of the knee (CPAK). total knee arthroplasty (TKA) can be an option for CPAK type II-aligned osteoarthritis in older inactive patients. Here, we hypothesized that joint line horizontalization by femoral-varus tibial-valgus osteotomy (FVTVO), which may reduce the shear stress induced by JLO, could be a treatment option for CPAK type II-aligned osteoarthritis in young active patients who wish to return to sports (RTS) activity. Our aim in this study was to evaluate the postoperative results of FVTVO with RTS.</p></div><div><h3>Methods</h3><p>Our indications for FVTVO are as follows: JLO >5°; mechanical medial proximal tibial angle (mMPTA) < 87°; mechanical lateral distal femoral angle (mLDFA) < 87°; typical osteoarthritis patterns for CPAK type II on magnetic resonance images, namely osteoarthritic change of the lateral tibial spine, medial slip of the femur, and/or lateral meniscal extrusion from the lateral femoral condyle; and flexion contracture <10°. We enrolled patients who wished to RTS and who had a pre-symptom Tegner score ≥5 and had completed at least a 1-year follow-up. For FVTVO, closed-wedge DFO was performed in all femurs; both closed-wedge HTO and open-wedge HTO were used in the tibia, depending on the situation. Range of motion exercises began on the first postoperative day, and full weight-bearing was permitted 6 weeks postoperatively. Jogging was permitted 3 months postoperatively after confirming bone union, and patients could gradually return to their sports activity 6–12 months’ postoperatively. The Japanese Orthopaedic Association (JOA) score and knee flexion range were assessed preoperatively and at the last follow-up. Tegner activity scale scores were assessed presymptom, preoperatively, and at the last follow-up. The hip-knee-ankle (HKA) angle, JLO, mMPTA, and mLDFA were evaluated radiologically, and meniscal extrusions, osteoarthritic change, and/or bone marrow edema were assessed on magnetic resonance images.</p></div><div><h3>Results</h3><p>One man and two women were included in this case series. Two were competitive athletes and one was a mountain climber. The patients' ages were 69, 46, and 57 years (Case 1, 2, and 3, respectively). All patients’ CPAK type was converted from type II to type V; i.e., neutral-aligned knee with a neutral joint line, postoperatively. All patients returned to their presymptom sports activity level by the final follow-up. The presymptom/preoperative/final follow-up Tegner scale in Case 1, 2, and 3 were 6/1/6, 5/2/5, and 7/3/7, respectively.</p></div><div><h3>Conclusion</h3><p>Joint line horizontalization by FVTVO for patients with a neutral-aligned knee with severe JLO provided highly satisfactory clinical results and successfully led to RTS.</p></div>","PeriodicalId":44283,"journal":{"name":"Asia-Pacific Journal of Sport Medicine Arthroscopy Rehabilitation and Technology","volume":"31 ","pages":"Pages 11-17"},"PeriodicalIF":1.4000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a9/f0/main.PMC9941361.pdf","citationCount":"2","resultStr":"{\"title\":\"Femoral-varus tibial-valgus osteotomy (FVTVO) for neutrally-aligned knee osteoarthritis with severe joint line obliquity enables return to sports activities: A case series study\",\"authors\":\"Ryuichi Nakamura , Masaki Amemiya , Tomoyuki Shimakawa , Masaki Takahashi , Kazunari Kuroda , Yasuo Katsuki , Akira Okano\",\"doi\":\"10.1016/j.asmart.2023.01.002\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Re-alignment surgeries for uni-compartmental knee osteoarthritis, such as high tibial osteotomy (HTO) for varus knees or distal femoral osteotomy (DFO) for valgus knees, are recognized as standard strategies. However, the treatment strategy has not been established for patients with a neutrally-aligned osteoarthritic knee with severe joint line obliquity (JLO) owing to the combination of a valgus femur and a varus tibia; i.e., type II coronal plane alignment of the knee (CPAK). total knee arthroplasty (TKA) can be an option for CPAK type II-aligned osteoarthritis in older inactive patients. Here, we hypothesized that joint line horizontalization by femoral-varus tibial-valgus osteotomy (FVTVO), which may reduce the shear stress induced by JLO, could be a treatment option for CPAK type II-aligned osteoarthritis in young active patients who wish to return to sports (RTS) activity. Our aim in this study was to evaluate the postoperative results of FVTVO with RTS.</p></div><div><h3>Methods</h3><p>Our indications for FVTVO are as follows: JLO >5°; mechanical medial proximal tibial angle (mMPTA) < 87°; mechanical lateral distal femoral angle (mLDFA) < 87°; typical osteoarthritis patterns for CPAK type II on magnetic resonance images, namely osteoarthritic change of the lateral tibial spine, medial slip of the femur, and/or lateral meniscal extrusion from the lateral femoral condyle; and flexion contracture <10°. We enrolled patients who wished to RTS and who had a pre-symptom Tegner score ≥5 and had completed at least a 1-year follow-up. For FVTVO, closed-wedge DFO was performed in all femurs; both closed-wedge HTO and open-wedge HTO were used in the tibia, depending on the situation. Range of motion exercises began on the first postoperative day, and full weight-bearing was permitted 6 weeks postoperatively. Jogging was permitted 3 months postoperatively after confirming bone union, and patients could gradually return to their sports activity 6–12 months’ postoperatively. The Japanese Orthopaedic Association (JOA) score and knee flexion range were assessed preoperatively and at the last follow-up. Tegner activity scale scores were assessed presymptom, preoperatively, and at the last follow-up. The hip-knee-ankle (HKA) angle, JLO, mMPTA, and mLDFA were evaluated radiologically, and meniscal extrusions, osteoarthritic change, and/or bone marrow edema were assessed on magnetic resonance images.</p></div><div><h3>Results</h3><p>One man and two women were included in this case series. Two were competitive athletes and one was a mountain climber. The patients' ages were 69, 46, and 57 years (Case 1, 2, and 3, respectively). All patients’ CPAK type was converted from type II to type V; i.e., neutral-aligned knee with a neutral joint line, postoperatively. All patients returned to their presymptom sports activity level by the final follow-up. The presymptom/preoperative/final follow-up Tegner scale in Case 1, 2, and 3 were 6/1/6, 5/2/5, and 7/3/7, respectively.</p></div><div><h3>Conclusion</h3><p>Joint line horizontalization by FVTVO for patients with a neutral-aligned knee with severe JLO provided highly satisfactory clinical results and successfully led to RTS.</p></div>\",\"PeriodicalId\":44283,\"journal\":{\"name\":\"Asia-Pacific Journal of Sport Medicine Arthroscopy Rehabilitation and Technology\",\"volume\":\"31 \",\"pages\":\"Pages 11-17\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a9/f0/main.PMC9941361.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Asia-Pacific Journal of Sport Medicine Arthroscopy Rehabilitation and Technology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S221468732300002X\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Asia-Pacific Journal of Sport Medicine Arthroscopy Rehabilitation and Technology","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S221468732300002X","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Femoral-varus tibial-valgus osteotomy (FVTVO) for neutrally-aligned knee osteoarthritis with severe joint line obliquity enables return to sports activities: A case series study
Background
Re-alignment surgeries for uni-compartmental knee osteoarthritis, such as high tibial osteotomy (HTO) for varus knees or distal femoral osteotomy (DFO) for valgus knees, are recognized as standard strategies. However, the treatment strategy has not been established for patients with a neutrally-aligned osteoarthritic knee with severe joint line obliquity (JLO) owing to the combination of a valgus femur and a varus tibia; i.e., type II coronal plane alignment of the knee (CPAK). total knee arthroplasty (TKA) can be an option for CPAK type II-aligned osteoarthritis in older inactive patients. Here, we hypothesized that joint line horizontalization by femoral-varus tibial-valgus osteotomy (FVTVO), which may reduce the shear stress induced by JLO, could be a treatment option for CPAK type II-aligned osteoarthritis in young active patients who wish to return to sports (RTS) activity. Our aim in this study was to evaluate the postoperative results of FVTVO with RTS.
Methods
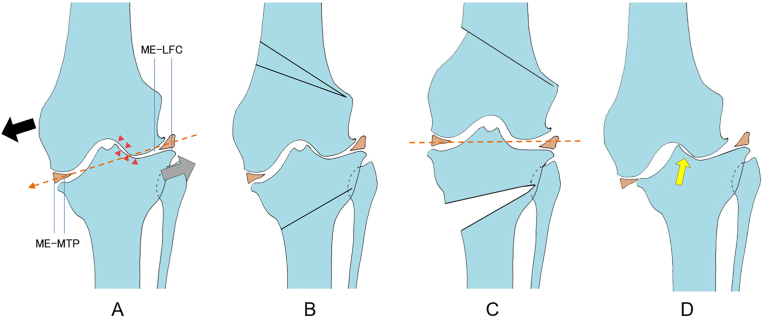
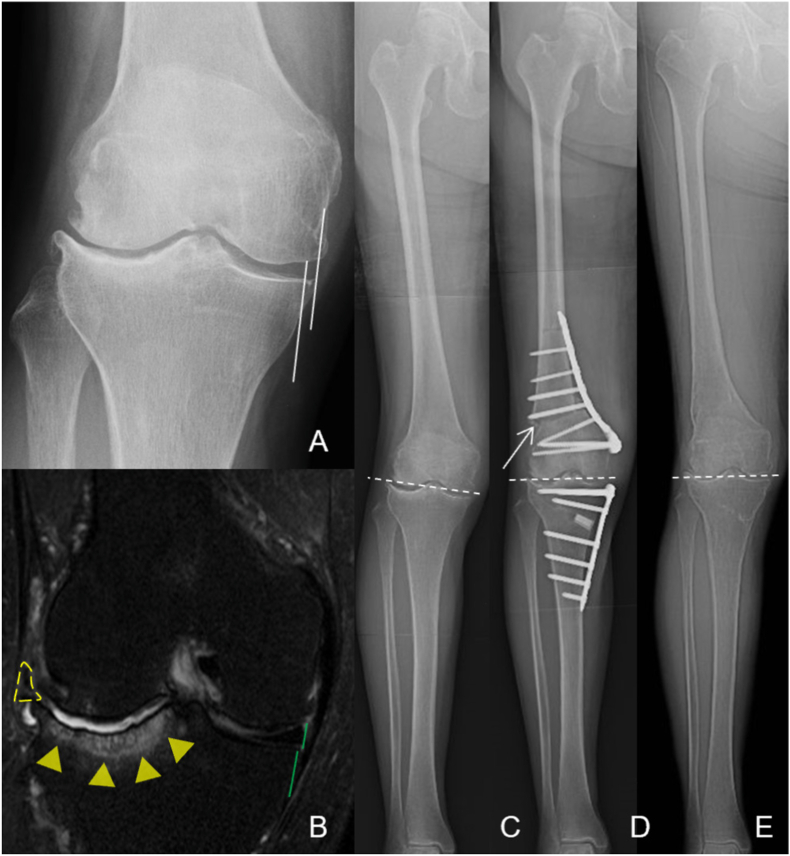
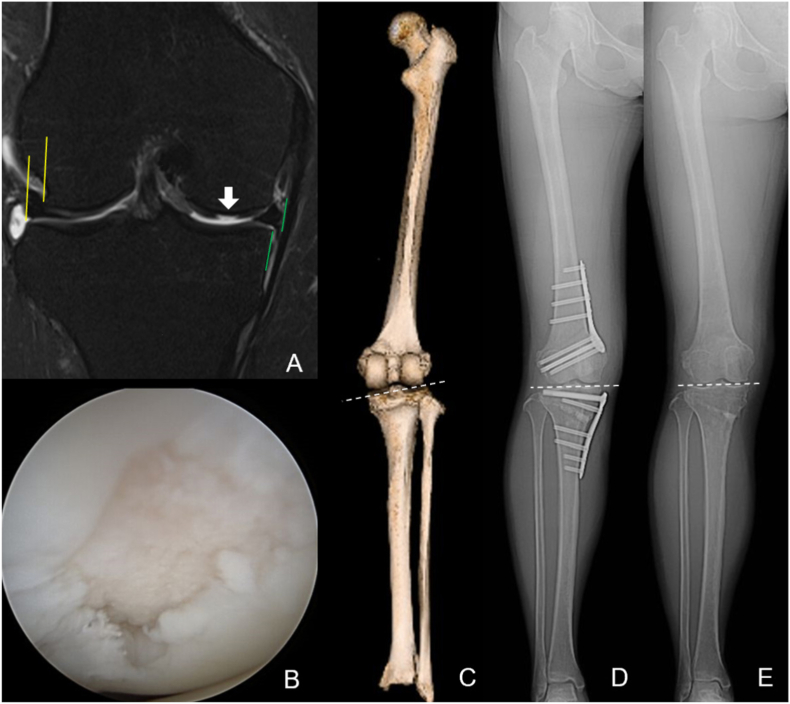
Our indications for FVTVO are as follows: JLO >5°; mechanical medial proximal tibial angle (mMPTA) < 87°; mechanical lateral distal femoral angle (mLDFA) < 87°; typical osteoarthritis patterns for CPAK type II on magnetic resonance images, namely osteoarthritic change of the lateral tibial spine, medial slip of the femur, and/or lateral meniscal extrusion from the lateral femoral condyle; and flexion contracture <10°. We enrolled patients who wished to RTS and who had a pre-symptom Tegner score ≥5 and had completed at least a 1-year follow-up. For FVTVO, closed-wedge DFO was performed in all femurs; both closed-wedge HTO and open-wedge HTO were used in the tibia, depending on the situation. Range of motion exercises began on the first postoperative day, and full weight-bearing was permitted 6 weeks postoperatively. Jogging was permitted 3 months postoperatively after confirming bone union, and patients could gradually return to their sports activity 6–12 months’ postoperatively. The Japanese Orthopaedic Association (JOA) score and knee flexion range were assessed preoperatively and at the last follow-up. Tegner activity scale scores were assessed presymptom, preoperatively, and at the last follow-up. The hip-knee-ankle (HKA) angle, JLO, mMPTA, and mLDFA were evaluated radiologically, and meniscal extrusions, osteoarthritic change, and/or bone marrow edema were assessed on magnetic resonance images.
Results
One man and two women were included in this case series. Two were competitive athletes and one was a mountain climber. The patients' ages were 69, 46, and 57 years (Case 1, 2, and 3, respectively). All patients’ CPAK type was converted from type II to type V; i.e., neutral-aligned knee with a neutral joint line, postoperatively. All patients returned to their presymptom sports activity level by the final follow-up. The presymptom/preoperative/final follow-up Tegner scale in Case 1, 2, and 3 were 6/1/6, 5/2/5, and 7/3/7, respectively.
Conclusion
Joint line horizontalization by FVTVO for patients with a neutral-aligned knee with severe JLO provided highly satisfactory clinical results and successfully led to RTS.
期刊介绍:
The Asia-Pacific Journal of Sports Medicine, Arthroscopy, Rehabilitation and Technology (AP-SMART) is the official peer-reviewed, open access journal of the Asia-Pacific Knee, Arthroscopy and Sports Medicine Society (APKASS) and the Japanese Orthopaedic Society of Knee, Arthroscopy and Sports Medicine (JOSKAS). It is published quarterly, in January, April, July and October, by Elsevier. The mission of AP-SMART is to inspire clinicians, practitioners, scientists and engineers to work towards a common goal to improve quality of life in the international community. The Journal publishes original research, reviews, editorials, perspectives, and letters to the Editor. Multidisciplinary research with collaboration amongst clinicians and scientists from different disciplines will be the trend in the coming decades. AP-SMART provides a platform for the exchange of new clinical and scientific information in the most precise and expeditious way to achieve timely dissemination of information and cross-fertilization of ideas.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


