Louiza S. Velentzis , David Hawkes , Michael Caruana , Julia ML. Brotherton , Megan A. Smith , Lara Roeske , Khurram A. Karim , Suzanne M. Garland , C. David Wrede , Jeffery Tan , Cosette Wheeler , Philip E. Castle , Marion Saville , Karen Canfell
{"title":"探索使用HPV初级筛查对HPV疫苗影响的人群监测策略","authors":"Louiza S. Velentzis , David Hawkes , Michael Caruana , Julia ML. Brotherton , Megan A. Smith , Lara Roeske , Khurram A. Karim , Suzanne M. Garland , C. David Wrede , Jeffery Tan , Cosette Wheeler , Philip E. Castle , Marion Saville , Karen Canfell","doi":"10.1016/j.tvr.2023.200255","DOIUrl":null,"url":null,"abstract":"<div><p>Australia's cervical screening program transitioned from cytology to HPV-testing with genotyping for HPV16/18 in Dec’2017. We investigated whether program data could be used to monitor HPV vaccination program impact (commenced in 2007) on HPV16/18 prevalence and compared estimates with pre-vaccination benchmark prevalence. Pre-vaccination samples (2005–2008) (n = 1933; WHINURS), from 25 to 64-year-old women had been previously analysed with Linear Array (LA). Post-vaccination samples (2013-2014) (n = 2989; Compass pilot), from 25 to 64-year-old women, were analysed by cobas 4800 (cobas), and by LA for historical comparability. Age standardised pre-vaccination HPV16/18 prevalence was 4.85% (95%CI:3.81–5.89) by LA; post-vaccination estimates were 1.67% (95%CI:1.21–2.13%) by LA, 1.49% (95%CI:1.05–1.93%) by cobas, and 1.63% (95%CI:1.17–2.08%) for cobas and LA testing of non-16/18 cobas positives (cobas/LA). Age-standardised pre-vaccination oncogenic HPV prevalence was 15.70% (95%CI:13.79–17.60%) by LA; post-vaccination estimates were 9.06% (95%CI:8.02–10.09%) by LA, 8.47% (95%CI:7.47–9.47%) by cobas and cobas/LA. Standardised rate ratios between post-vs. pre-vaccination rates were significantly different for HPV16/18, non-16/18 HPV and oncogenic HPV: 0.34 (95%CI:0.23–0.50), 0.68 (95%CI:0.55–0.84) and 0.58 (95%CI:0.48–0.69), respectively. Additional strategies (LA for all cobas positives; combined cobas and LA results on all samples) had similar results. If a single method is applied consistently, it will provide important data on relative changes in HPV prevalence following vaccination.</p></div>","PeriodicalId":52381,"journal":{"name":"Tumour Virus Research","volume":"15 ","pages":"Article 200255"},"PeriodicalIF":8.1000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f1/c2/main.PMC9925607.pdf","citationCount":"0","resultStr":"{\"title\":\"Exploring monitoring strategies for population surveillance of HPV vaccine impact using primary HPV screening\",\"authors\":\"Louiza S. Velentzis , David Hawkes , Michael Caruana , Julia ML. Brotherton , Megan A. Smith , Lara Roeske , Khurram A. Karim , Suzanne M. Garland , C. David Wrede , Jeffery Tan , Cosette Wheeler , Philip E. Castle , Marion Saville , Karen Canfell\",\"doi\":\"10.1016/j.tvr.2023.200255\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><p>Australia's cervical screening program transitioned from cytology to HPV-testing with genotyping for HPV16/18 in Dec’2017. We investigated whether program data could be used to monitor HPV vaccination program impact (commenced in 2007) on HPV16/18 prevalence and compared estimates with pre-vaccination benchmark prevalence. Pre-vaccination samples (2005–2008) (n = 1933; WHINURS), from 25 to 64-year-old women had been previously analysed with Linear Array (LA). Post-vaccination samples (2013-2014) (n = 2989; Compass pilot), from 25 to 64-year-old women, were analysed by cobas 4800 (cobas), and by LA for historical comparability. Age standardised pre-vaccination HPV16/18 prevalence was 4.85% (95%CI:3.81–5.89) by LA; post-vaccination estimates were 1.67% (95%CI:1.21–2.13%) by LA, 1.49% (95%CI:1.05–1.93%) by cobas, and 1.63% (95%CI:1.17–2.08%) for cobas and LA testing of non-16/18 cobas positives (cobas/LA). Age-standardised pre-vaccination oncogenic HPV prevalence was 15.70% (95%CI:13.79–17.60%) by LA; post-vaccination estimates were 9.06% (95%CI:8.02–10.09%) by LA, 8.47% (95%CI:7.47–9.47%) by cobas and cobas/LA. Standardised rate ratios between post-vs. pre-vaccination rates were significantly different for HPV16/18, non-16/18 HPV and oncogenic HPV: 0.34 (95%CI:0.23–0.50), 0.68 (95%CI:0.55–0.84) and 0.58 (95%CI:0.48–0.69), respectively. Additional strategies (LA for all cobas positives; combined cobas and LA results on all samples) had similar results. If a single method is applied consistently, it will provide important data on relative changes in HPV prevalence following vaccination.</p></div>\",\"PeriodicalId\":52381,\"journal\":{\"name\":\"Tumour Virus Research\",\"volume\":\"15 \",\"pages\":\"Article 200255\"},\"PeriodicalIF\":8.1000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f1/c2/main.PMC9925607.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Tumour Virus Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2666679023000022\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"VIROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tumour Virus Research","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666679023000022","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"VIROLOGY","Score":null,"Total":0}
Exploring monitoring strategies for population surveillance of HPV vaccine impact using primary HPV screening
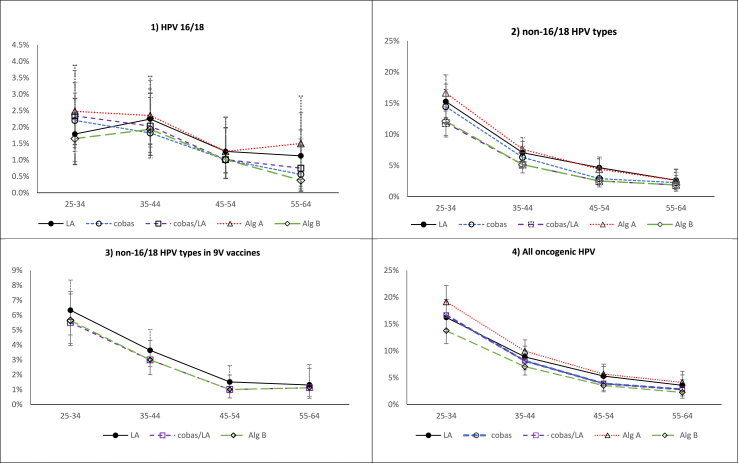
Australia's cervical screening program transitioned from cytology to HPV-testing with genotyping for HPV16/18 in Dec’2017. We investigated whether program data could be used to monitor HPV vaccination program impact (commenced in 2007) on HPV16/18 prevalence and compared estimates with pre-vaccination benchmark prevalence. Pre-vaccination samples (2005–2008) (n = 1933; WHINURS), from 25 to 64-year-old women had been previously analysed with Linear Array (LA). Post-vaccination samples (2013-2014) (n = 2989; Compass pilot), from 25 to 64-year-old women, were analysed by cobas 4800 (cobas), and by LA for historical comparability. Age standardised pre-vaccination HPV16/18 prevalence was 4.85% (95%CI:3.81–5.89) by LA; post-vaccination estimates were 1.67% (95%CI:1.21–2.13%) by LA, 1.49% (95%CI:1.05–1.93%) by cobas, and 1.63% (95%CI:1.17–2.08%) for cobas and LA testing of non-16/18 cobas positives (cobas/LA). Age-standardised pre-vaccination oncogenic HPV prevalence was 15.70% (95%CI:13.79–17.60%) by LA; post-vaccination estimates were 9.06% (95%CI:8.02–10.09%) by LA, 8.47% (95%CI:7.47–9.47%) by cobas and cobas/LA. Standardised rate ratios between post-vs. pre-vaccination rates were significantly different for HPV16/18, non-16/18 HPV and oncogenic HPV: 0.34 (95%CI:0.23–0.50), 0.68 (95%CI:0.55–0.84) and 0.58 (95%CI:0.48–0.69), respectively. Additional strategies (LA for all cobas positives; combined cobas and LA results on all samples) had similar results. If a single method is applied consistently, it will provide important data on relative changes in HPV prevalence following vaccination.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


