Stephen S DiGiovanni, Rebecca J Hoffmann Frances, Rebecca S Brown, Barrett T Wilkinson, Gillian E Coates, Laura J Faherty, Alexa K Craig, Elizabeth R Andrews, Sarah M B Gabrielson
{"title":"儿童创伤和创伤后症状筛查在健康儿童访问。","authors":"Stephen S DiGiovanni, Rebecca J Hoffmann Frances, Rebecca S Brown, Barrett T Wilkinson, Gillian E Coates, Laura J Faherty, Alexa K Craig, Elizabeth R Andrews, Sarah M B Gabrielson","doi":"10.1097/pq9.0000000000000640","DOIUrl":null,"url":null,"abstract":"<p><p>Adverse childhood experiences (ACEs), including abuse or neglect, parental substance abuse, mental illness, or separation, are public health crises that require identification and response. We aimed to increase annual rates of trauma screening during well-child visits from 0% to 70%, post-traumatic stress disorder (PTSD) symptom screening for children with identified trauma from 0% to 30%, and connection to behavioral health for children with symptoms from 0% to 60%.</p><p><strong>Methods: </strong>Our interdisciplinary behavioral and medical health team implemented 3 plan-do-study-act cycles to improve screening and response to pediatric traumatic experiences. Automated reports and chart reviews measured progress toward goals as we changed screening methods and provider training.</p><p><strong>Results: </strong>During plan-do-study-act cycle 1, a chart review of patients with positive trauma screenings identified various trauma types. During cycle 2, a comparison of screening methods demonstrated that written screening identified trauma among more children than verbal screening (8.3% versus 1.7%). During cycle 3, practices completed trauma screenings at 25,287 (89.8%) well-child visits. Among screenings, 2,441 (9.7%) identified trauma. The abbreviated Post Traumatic Stress Disorder Reaction Index was conducted at 907 (37.2%) encounters and identified 520 children (57.3%) with PTSD symptoms. Among a sample of 250, 26.4% were referred to behavioral health, 43.2% were already connected, and 30.4% had no connection.</p><p><strong>Conclusions: </strong>It is feasible to screen and respond to trauma during well-child visits. Screening method and training implementation changes can improve screening and response to pediatric trauma and PTSD. Further work is needed to increase rates of PTSD symptomology screening and connection to behavioral health.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"8 3","pages":"e640"},"PeriodicalIF":1.2000,"publicationDate":"2023-05-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/64/53/pqs-8-e640.PMC10219716.pdf","citationCount":"1","resultStr":"{\"title\":\"Pediatric Trauma and Posttraumatic Symptom Screening at Well-child Visits.\",\"authors\":\"Stephen S DiGiovanni, Rebecca J Hoffmann Frances, Rebecca S Brown, Barrett T Wilkinson, Gillian E Coates, Laura J Faherty, Alexa K Craig, Elizabeth R Andrews, Sarah M B Gabrielson\",\"doi\":\"10.1097/pq9.0000000000000640\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Adverse childhood experiences (ACEs), including abuse or neglect, parental substance abuse, mental illness, or separation, are public health crises that require identification and response. We aimed to increase annual rates of trauma screening during well-child visits from 0% to 70%, post-traumatic stress disorder (PTSD) symptom screening for children with identified trauma from 0% to 30%, and connection to behavioral health for children with symptoms from 0% to 60%.</p><p><strong>Methods: </strong>Our interdisciplinary behavioral and medical health team implemented 3 plan-do-study-act cycles to improve screening and response to pediatric traumatic experiences. Automated reports and chart reviews measured progress toward goals as we changed screening methods and provider training.</p><p><strong>Results: </strong>During plan-do-study-act cycle 1, a chart review of patients with positive trauma screenings identified various trauma types. During cycle 2, a comparison of screening methods demonstrated that written screening identified trauma among more children than verbal screening (8.3% versus 1.7%). During cycle 3, practices completed trauma screenings at 25,287 (89.8%) well-child visits. Among screenings, 2,441 (9.7%) identified trauma. The abbreviated Post Traumatic Stress Disorder Reaction Index was conducted at 907 (37.2%) encounters and identified 520 children (57.3%) with PTSD symptoms. Among a sample of 250, 26.4% were referred to behavioral health, 43.2% were already connected, and 30.4% had no connection.</p><p><strong>Conclusions: </strong>It is feasible to screen and respond to trauma during well-child visits. Screening method and training implementation changes can improve screening and response to pediatric trauma and PTSD. Further work is needed to increase rates of PTSD symptomology screening and connection to behavioral health.</p>\",\"PeriodicalId\":74412,\"journal\":{\"name\":\"Pediatric quality & safety\",\"volume\":\"8 3\",\"pages\":\"e640\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2023-05-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/64/53/pqs-8-e640.PMC10219716.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric quality & safety\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/pq9.0000000000000640\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/5/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000640","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/5/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
Pediatric Trauma and Posttraumatic Symptom Screening at Well-child Visits.
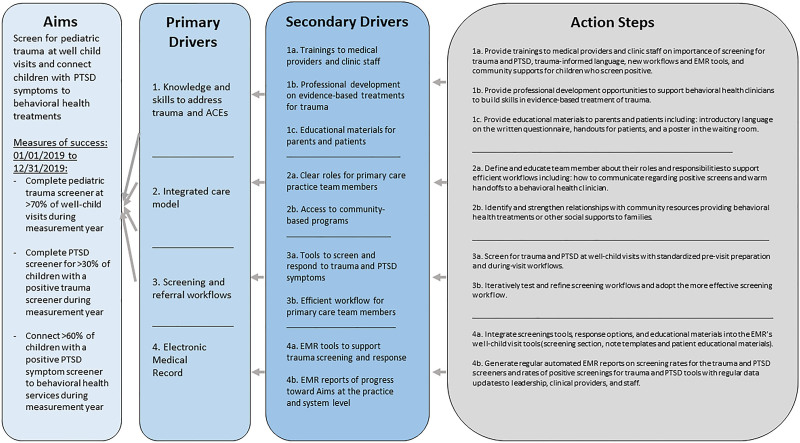
Adverse childhood experiences (ACEs), including abuse or neglect, parental substance abuse, mental illness, or separation, are public health crises that require identification and response. We aimed to increase annual rates of trauma screening during well-child visits from 0% to 70%, post-traumatic stress disorder (PTSD) symptom screening for children with identified trauma from 0% to 30%, and connection to behavioral health for children with symptoms from 0% to 60%.
Methods: Our interdisciplinary behavioral and medical health team implemented 3 plan-do-study-act cycles to improve screening and response to pediatric traumatic experiences. Automated reports and chart reviews measured progress toward goals as we changed screening methods and provider training.
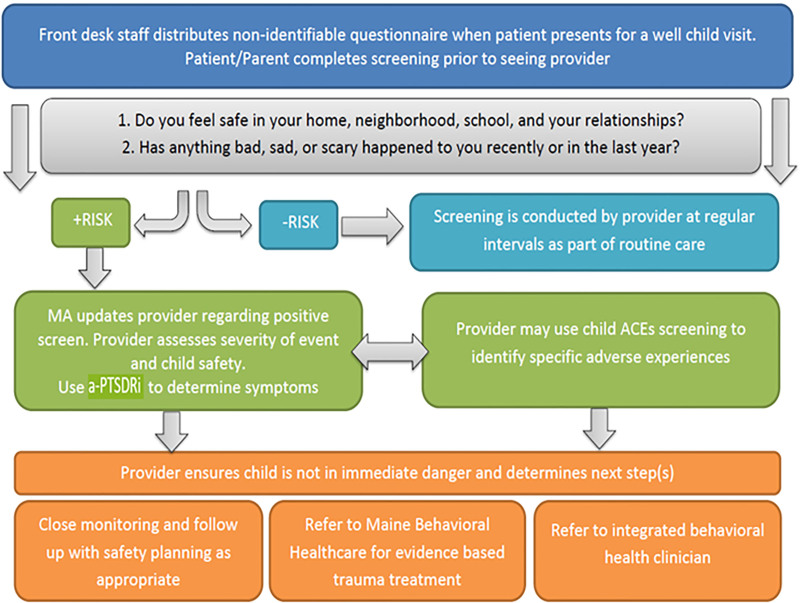
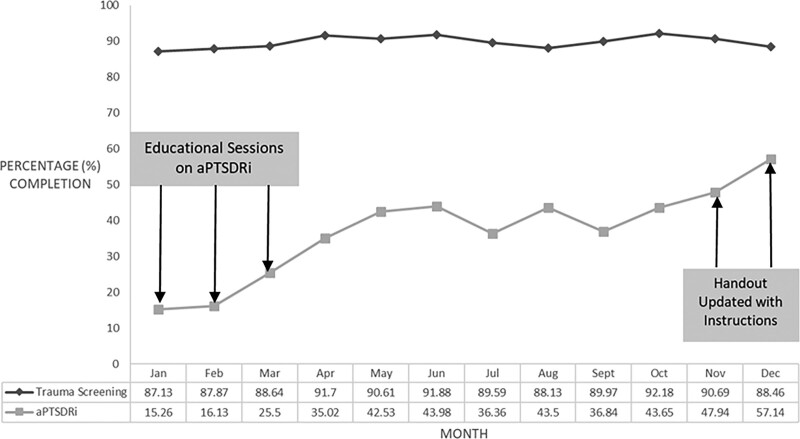
Results: During plan-do-study-act cycle 1, a chart review of patients with positive trauma screenings identified various trauma types. During cycle 2, a comparison of screening methods demonstrated that written screening identified trauma among more children than verbal screening (8.3% versus 1.7%). During cycle 3, practices completed trauma screenings at 25,287 (89.8%) well-child visits. Among screenings, 2,441 (9.7%) identified trauma. The abbreviated Post Traumatic Stress Disorder Reaction Index was conducted at 907 (37.2%) encounters and identified 520 children (57.3%) with PTSD symptoms. Among a sample of 250, 26.4% were referred to behavioral health, 43.2% were already connected, and 30.4% had no connection.
Conclusions: It is feasible to screen and respond to trauma during well-child visits. Screening method and training implementation changes can improve screening and response to pediatric trauma and PTSD. Further work is needed to increase rates of PTSD symptomology screening and connection to behavioral health.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


