{"title":"乳腺闪烁成像在可疑(乳腺影像报告与数据系统IV)乳腺病变中的应用。","authors":"Ali Reza Azarpeikan, Ramesh Omranipour, Habibollah Mahmoodzadeh, Seyed Rouhollah Miri, Narjes Mohammadzadeh, Farhang Derakhshan, Saeed Farzanefar, Mehrshad Abbasi","doi":"10.4103/abr.abr_347_21","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The surgery for a breast imaging-reporting and data system (BIRADS) IV lesions needs imaging or pathology supporting data. The roll of breast scintigraphy for this purpose is unclear.</p><p><strong>Materials and methods: </strong>In a prospective design, 16 patients with 25 BIRADS IV lesions who were scheduled for surgery were included. Before the surgery, breast scintigraphy was done using a nondedicated dual head gamma camera in the prone position employing a shaped foam pad providing imaging at breast pendulous position. Twenty mCi<sup>99m</sup> Tc methoxy-isobutyl-isonitrile was injected and two 15 and 60-min delayed imaging were done (anterior, bilateral, and single photon emission computed tomography [SPECT] projections). Pathology reports were collected and tumor to nontumor uptake ratio (T/NT) was analyzed, accordingly.</p><p><strong>Results: </strong>Out of all lesions, 12 were malignant (invasive ductal and lobular carcinoma ductal carcinoma <i>in situ</i>). At 15 min, T/NT was insignificantly higher in the malignant compared to benign lesions (22.8 ± 23.9 vs. 10.1 ± 10.1; <i>P</i> = 0.109). The optimal T/NT cutoff for discrimination of malignant and benign lesions was 20. Only 1 out of 13 benign lesions presented uptake >20 (7.7%; false-positive rate; <i>P</i> = 0.047). The diagnostic accuracy, sensitivity, and specificity for T/NT calculated at 0.68, 0.42, and 0.92, respectively. The T/NT at 60 min remained unchanged for either benign or malignant lesions (22.3 ± 30.2 vs. 11.7 ± 17.1; <i>P</i> = 0.296).</p><p><strong>Conclusions: </strong>Breast scintigraphy with general purpose gamma camera employing SPECT imaging may assist the selection of BIRADS IV lesions in need for surgery. All uptake positive cases should undergo surgery and decision for uptake negative cases should be made based on other data.</p>","PeriodicalId":7225,"journal":{"name":"Advanced Biomedical Research","volume":"12 ","pages":"86"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/57/d5/ABR-12-86.PMC10241632.pdf","citationCount":"0","resultStr":"{\"title\":\"Application of Breast Scintigraphy for Patients with Suspicious (Breast Imaging-Reporting and Data System IV) Breast Lesions.\",\"authors\":\"Ali Reza Azarpeikan, Ramesh Omranipour, Habibollah Mahmoodzadeh, Seyed Rouhollah Miri, Narjes Mohammadzadeh, Farhang Derakhshan, Saeed Farzanefar, Mehrshad Abbasi\",\"doi\":\"10.4103/abr.abr_347_21\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The surgery for a breast imaging-reporting and data system (BIRADS) IV lesions needs imaging or pathology supporting data. The roll of breast scintigraphy for this purpose is unclear.</p><p><strong>Materials and methods: </strong>In a prospective design, 16 patients with 25 BIRADS IV lesions who were scheduled for surgery were included. Before the surgery, breast scintigraphy was done using a nondedicated dual head gamma camera in the prone position employing a shaped foam pad providing imaging at breast pendulous position. Twenty mCi<sup>99m</sup> Tc methoxy-isobutyl-isonitrile was injected and two 15 and 60-min delayed imaging were done (anterior, bilateral, and single photon emission computed tomography [SPECT] projections). Pathology reports were collected and tumor to nontumor uptake ratio (T/NT) was analyzed, accordingly.</p><p><strong>Results: </strong>Out of all lesions, 12 were malignant (invasive ductal and lobular carcinoma ductal carcinoma <i>in situ</i>). At 15 min, T/NT was insignificantly higher in the malignant compared to benign lesions (22.8 ± 23.9 vs. 10.1 ± 10.1; <i>P</i> = 0.109). The optimal T/NT cutoff for discrimination of malignant and benign lesions was 20. Only 1 out of 13 benign lesions presented uptake >20 (7.7%; false-positive rate; <i>P</i> = 0.047). The diagnostic accuracy, sensitivity, and specificity for T/NT calculated at 0.68, 0.42, and 0.92, respectively. The T/NT at 60 min remained unchanged for either benign or malignant lesions (22.3 ± 30.2 vs. 11.7 ± 17.1; <i>P</i> = 0.296).</p><p><strong>Conclusions: </strong>Breast scintigraphy with general purpose gamma camera employing SPECT imaging may assist the selection of BIRADS IV lesions in need for surgery. All uptake positive cases should undergo surgery and decision for uptake negative cases should be made based on other data.</p>\",\"PeriodicalId\":7225,\"journal\":{\"name\":\"Advanced Biomedical Research\",\"volume\":\"12 \",\"pages\":\"86\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/57/d5/ABR-12-86.PMC10241632.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Advanced Biomedical Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/abr.abr_347_21\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advanced Biomedical Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/abr.abr_347_21","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Application of Breast Scintigraphy for Patients with Suspicious (Breast Imaging-Reporting and Data System IV) Breast Lesions.
Background: The surgery for a breast imaging-reporting and data system (BIRADS) IV lesions needs imaging or pathology supporting data. The roll of breast scintigraphy for this purpose is unclear.
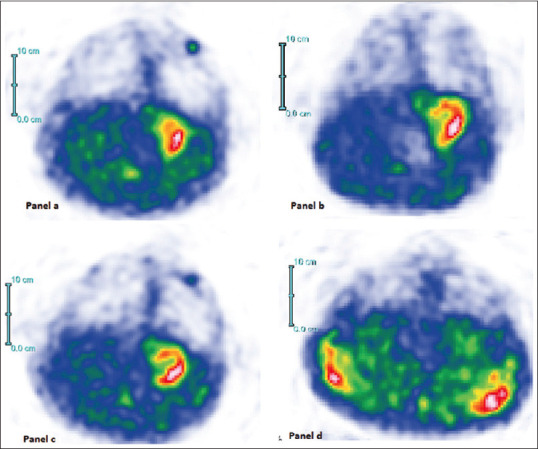
Materials and methods: In a prospective design, 16 patients with 25 BIRADS IV lesions who were scheduled for surgery were included. Before the surgery, breast scintigraphy was done using a nondedicated dual head gamma camera in the prone position employing a shaped foam pad providing imaging at breast pendulous position. Twenty mCi99m Tc methoxy-isobutyl-isonitrile was injected and two 15 and 60-min delayed imaging were done (anterior, bilateral, and single photon emission computed tomography [SPECT] projections). Pathology reports were collected and tumor to nontumor uptake ratio (T/NT) was analyzed, accordingly.
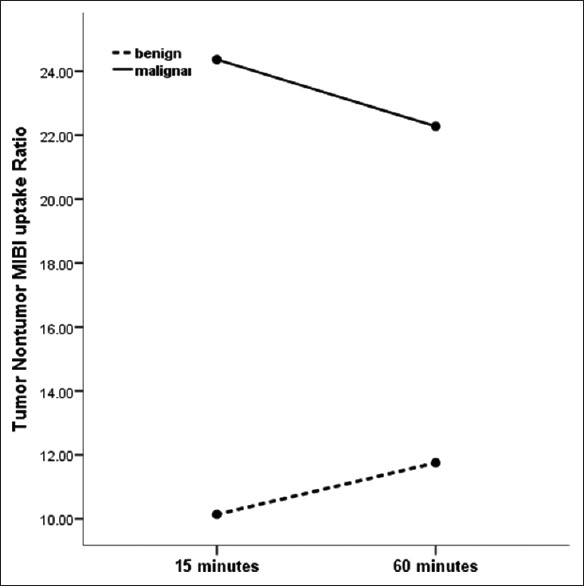
Results: Out of all lesions, 12 were malignant (invasive ductal and lobular carcinoma ductal carcinoma in situ). At 15 min, T/NT was insignificantly higher in the malignant compared to benign lesions (22.8 ± 23.9 vs. 10.1 ± 10.1; P = 0.109). The optimal T/NT cutoff for discrimination of malignant and benign lesions was 20. Only 1 out of 13 benign lesions presented uptake >20 (7.7%; false-positive rate; P = 0.047). The diagnostic accuracy, sensitivity, and specificity for T/NT calculated at 0.68, 0.42, and 0.92, respectively. The T/NT at 60 min remained unchanged for either benign or malignant lesions (22.3 ± 30.2 vs. 11.7 ± 17.1; P = 0.296).
Conclusions: Breast scintigraphy with general purpose gamma camera employing SPECT imaging may assist the selection of BIRADS IV lesions in need for surgery. All uptake positive cases should undergo surgery and decision for uptake negative cases should be made based on other data.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


