Amir Sarayani, Joshua D Brown, Christian Hampp, William T Donahoo, Almut G Winterstein
{"title":"美国医疗系统从ICD-9向ICD-10过渡中高维倾向评分程序的适应性","authors":"Amir Sarayani, Joshua D Brown, Christian Hampp, William T Donahoo, Almut G Winterstein","doi":"10.2147/CLEP.S405165","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>High-Dimensional Propensity Score procedure (HDPS) is a data-driven approach to assist control for confounding in pharmacoepidemiologic research. The transition to the International Classification of Disease (ICD-9/10) in the US health system may pose uncertainty in applying the HDPS procedure.</p><p><strong>Methods: </strong>We assembled a base cohort of patients in MarketScan<sup>®</sup> Commercial Claims Database who had newly initiated celecoxib or traditional NSAIDs to compare gastrointestinal bleeding risk. We then created bootstrapped hypothetical cohorts from the base cohort with predefined patient selection patterns from the ICD eras. Three strategies for HDPS deployment were tested: 1) split the cohort by ICD era, deploy HDPS twice, and pool the relative risks (pooled RR), 2) consider codes from each ICD era as a separate data dimension and deploy HDPS in the entire cohort (data dimensions) and 3) map ICD codes from both eras to Clinical Classifications Software (CCS) concepts before deploying HDPS in the entire cohort (CCS mapping). We calculated percent bias and root-mean-squared error to compare the strategies.</p><p><strong>Results: </strong>A similar bias reduction was observed in cohorts where patient selection pattern from each ICD era was comparable between the exposure groups. In the presence of considerable disparity in patient selection, we observed a bimodal distribution of propensity scores in the data dimensions strategy, indicating instrument-like covariates. Moreover, the CCS mapping strategy resulted in at least 30% less bias than pooled RR and data dimensions strategies (RMSE: 0.14, 0.19, 0.21, respectively) in this scenario.</p><p><strong>Conclusion: </strong>Mapping ICD codes to a stable terminology like CCS serves as a helpful strategy to reduce residual bias when deploying HDPS in pharmacoepidemiologic studies spanning both ICD eras.</p>","PeriodicalId":10362,"journal":{"name":"Clinical Epidemiology","volume":null,"pages":null},"PeriodicalIF":3.4000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b0/00/clep-15-645.PMC10237200.pdf","citationCount":"0","resultStr":"{\"title\":\"Adaptability of High Dimensional Propensity Score Procedure in the Transition from ICD-9 to ICD-10 in the US Healthcare System.\",\"authors\":\"Amir Sarayani, Joshua D Brown, Christian Hampp, William T Donahoo, Almut G Winterstein\",\"doi\":\"10.2147/CLEP.S405165\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>High-Dimensional Propensity Score procedure (HDPS) is a data-driven approach to assist control for confounding in pharmacoepidemiologic research. The transition to the International Classification of Disease (ICD-9/10) in the US health system may pose uncertainty in applying the HDPS procedure.</p><p><strong>Methods: </strong>We assembled a base cohort of patients in MarketScan<sup>®</sup> Commercial Claims Database who had newly initiated celecoxib or traditional NSAIDs to compare gastrointestinal bleeding risk. We then created bootstrapped hypothetical cohorts from the base cohort with predefined patient selection patterns from the ICD eras. Three strategies for HDPS deployment were tested: 1) split the cohort by ICD era, deploy HDPS twice, and pool the relative risks (pooled RR), 2) consider codes from each ICD era as a separate data dimension and deploy HDPS in the entire cohort (data dimensions) and 3) map ICD codes from both eras to Clinical Classifications Software (CCS) concepts before deploying HDPS in the entire cohort (CCS mapping). We calculated percent bias and root-mean-squared error to compare the strategies.</p><p><strong>Results: </strong>A similar bias reduction was observed in cohorts where patient selection pattern from each ICD era was comparable between the exposure groups. In the presence of considerable disparity in patient selection, we observed a bimodal distribution of propensity scores in the data dimensions strategy, indicating instrument-like covariates. Moreover, the CCS mapping strategy resulted in at least 30% less bias than pooled RR and data dimensions strategies (RMSE: 0.14, 0.19, 0.21, respectively) in this scenario.</p><p><strong>Conclusion: </strong>Mapping ICD codes to a stable terminology like CCS serves as a helpful strategy to reduce residual bias when deploying HDPS in pharmacoepidemiologic studies spanning both ICD eras.</p>\",\"PeriodicalId\":10362,\"journal\":{\"name\":\"Clinical Epidemiology\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b0/00/clep-15-645.PMC10237200.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Epidemiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/CLEP.S405165\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Epidemiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/CLEP.S405165","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
Adaptability of High Dimensional Propensity Score Procedure in the Transition from ICD-9 to ICD-10 in the US Healthcare System.
Background: High-Dimensional Propensity Score procedure (HDPS) is a data-driven approach to assist control for confounding in pharmacoepidemiologic research. The transition to the International Classification of Disease (ICD-9/10) in the US health system may pose uncertainty in applying the HDPS procedure.
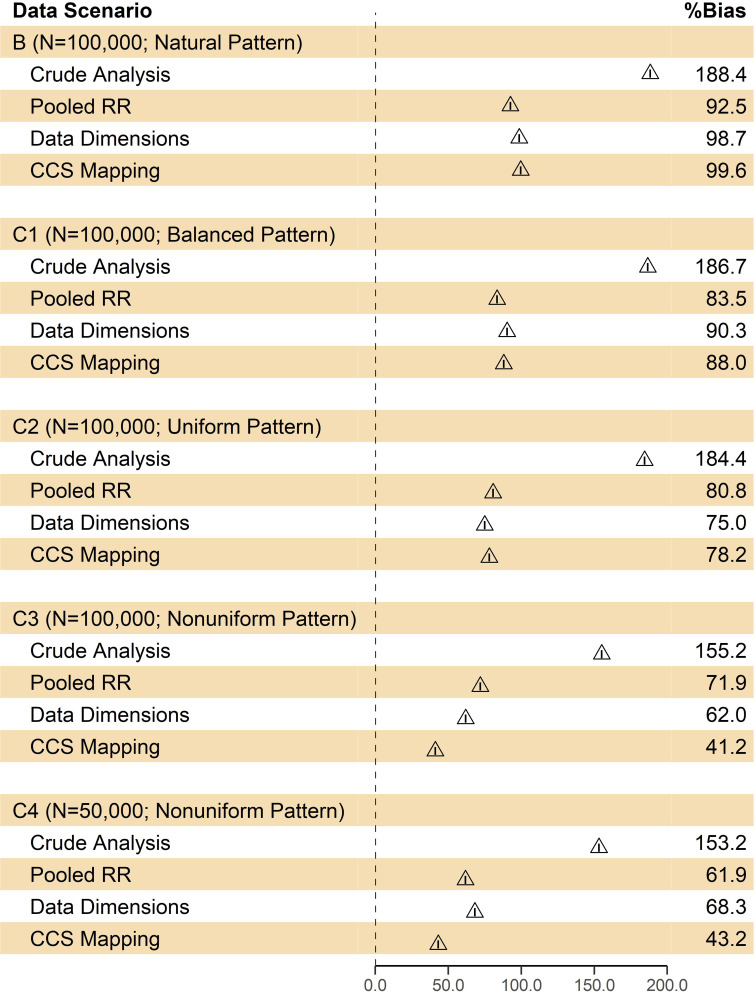
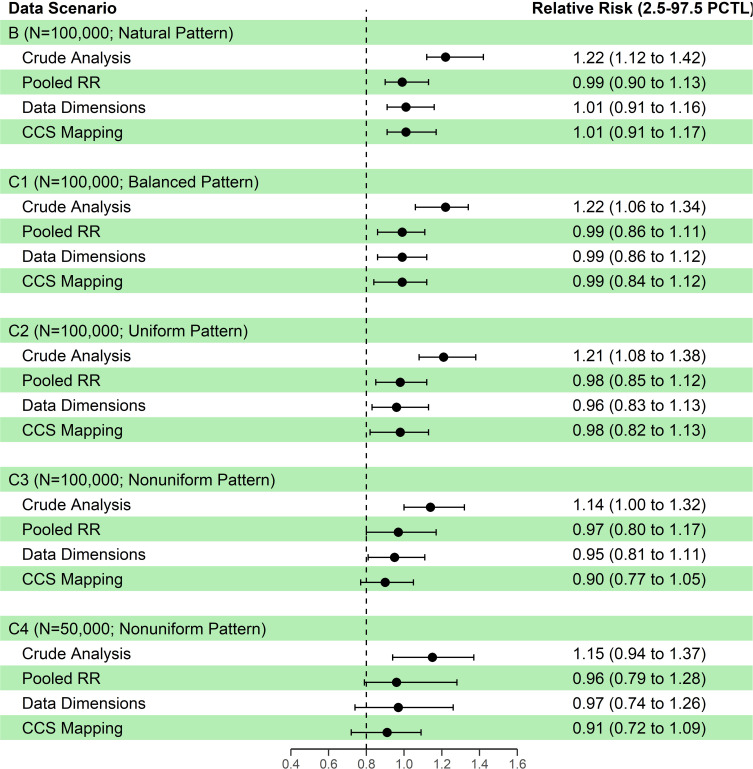
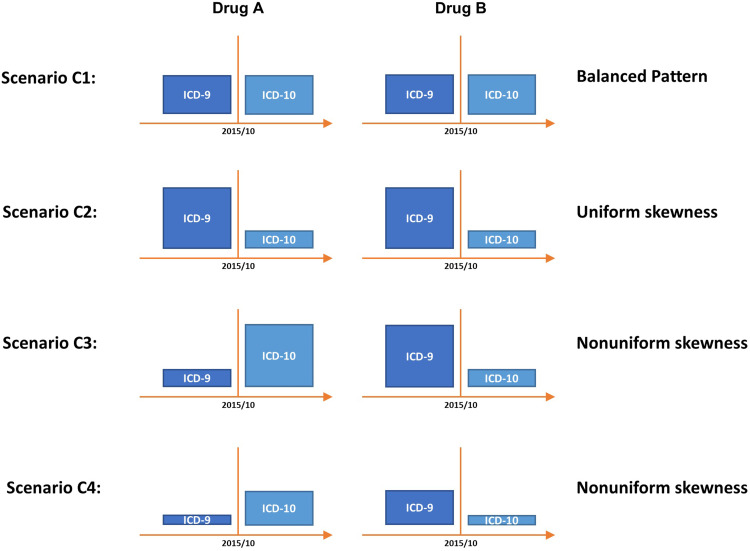
Methods: We assembled a base cohort of patients in MarketScan® Commercial Claims Database who had newly initiated celecoxib or traditional NSAIDs to compare gastrointestinal bleeding risk. We then created bootstrapped hypothetical cohorts from the base cohort with predefined patient selection patterns from the ICD eras. Three strategies for HDPS deployment were tested: 1) split the cohort by ICD era, deploy HDPS twice, and pool the relative risks (pooled RR), 2) consider codes from each ICD era as a separate data dimension and deploy HDPS in the entire cohort (data dimensions) and 3) map ICD codes from both eras to Clinical Classifications Software (CCS) concepts before deploying HDPS in the entire cohort (CCS mapping). We calculated percent bias and root-mean-squared error to compare the strategies.
Results: A similar bias reduction was observed in cohorts where patient selection pattern from each ICD era was comparable between the exposure groups. In the presence of considerable disparity in patient selection, we observed a bimodal distribution of propensity scores in the data dimensions strategy, indicating instrument-like covariates. Moreover, the CCS mapping strategy resulted in at least 30% less bias than pooled RR and data dimensions strategies (RMSE: 0.14, 0.19, 0.21, respectively) in this scenario.
Conclusion: Mapping ICD codes to a stable terminology like CCS serves as a helpful strategy to reduce residual bias when deploying HDPS in pharmacoepidemiologic studies spanning both ICD eras.
期刊介绍:
Clinical Epidemiology is an international, peer reviewed, open access journal. Clinical Epidemiology focuses on the application of epidemiological principles and questions relating to patients and clinical care in terms of prevention, diagnosis, prognosis, and treatment.
Clinical Epidemiology welcomes papers covering these topics in form of original research and systematic reviews.
Clinical Epidemiology has a special interest in international electronic medical patient records and other routine health care data, especially as applied to safety of medical interventions, clinical utility of diagnostic procedures, understanding short- and long-term clinical course of diseases, clinical epidemiological and biostatistical methods, and systematic reviews.
When considering submission of a paper utilizing publicly-available data, authors should ensure that such studies add significantly to the body of knowledge and that they use appropriate validated methods for identifying health outcomes.
The journal has launched special series describing existing data sources for clinical epidemiology, international health care systems and validation studies of algorithms based on databases and registries.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


