Lita Araujo, Srikanth Kyatham, Kristen G Bzdek, Keiko Higuchi, Nupur Greene
{"title":"评估美国商业保险多发性硬化症复发患者从其他疾病改善治疗转向特立氟米特的健康经济结果。","authors":"Lita Araujo, Srikanth Kyatham, Kristen G Bzdek, Keiko Higuchi, Nupur Greene","doi":"10.2147/CEOR.S401687","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Assess patient characteristics, healthcare resource utilization (HCRU), and relapses in patients with multiple sclerosis (MS) who switched to teriflunomide from other disease-modifying therapies (DMTs).</p><p><strong>Methods: </strong>Retrospective study of US Merative™ MarketScan<sup>®</sup> claims database (Jan 1, 2012-July 31, 2020,) including HIPAA-compliant, deidentified data. Patients ≥18 years with MS diagnosis (based on ICD-9/ICD-10 codes), receiving ≥1 DMT prior to teriflunomide and ≥12 months continuous enrollment pre and post index (date of teriflunomide initiation). Outcomes included inpatient and emergency room claims coinciding with MS diagnosis, MS-related healthcare costs, and annualized relapse rates (ARRs) (indirectly assessed using hospitalization/outpatient claims and steroid use coinciding with MS diagnosis).</p><p><strong>Results: </strong>The analyzed cohort (N=2016) was primarily female (79%); age (mean ± standard deviation) 51.4 ± 9.3 years; MS duration 4.7±2.8 years (at index). The majority (89.2%) were treated with one DMT before switching to teriflunomide. Use of outpatient services (event rate/100 person-years) increased post vs pre index; however, MRI visits significantly reduced over the same period (both <i>P</i><0.0001). Costs for MS-specific outpatient visits decreased by $371 per patient per year (PPPY) after switching to teriflunomide. Despite an increase in use post index (0.024 to 0.033 rate/100 person-years; <i>P</i><0.0001), costs for MS-specific laboratory services reduced (pre-index: $271 vs $248 PPPY post-index; <i>P</i>=0.02). Fewer patients had relapses after switching (pre-index: n=417 [20.7%]; post-index: n=333 [16.5%]). ARR was significantly lower after switching (pre-index: 0.269 vs post-index: 0.205; <i>P</i>=0.000).</p><p><strong>Conclusion: </strong>Switching to teriflunomide from existing DMTs in patients with relapsing MS resulted in a reduction in outpatient HCRU in this analysis of US claims data. The real-world effectiveness of teriflunomide was generally consistent with efficacy reported in clinical trials, showing a reduction in relapse following a switch to teriflunomide.</p>","PeriodicalId":47313,"journal":{"name":"ClinicoEconomics and Outcomes Research","volume":null,"pages":null},"PeriodicalIF":2.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e2/59/ceor-15-361.PMC10208242.pdf","citationCount":"0","resultStr":"{\"title\":\"Assessing the Health Economic Outcomes from Commercially Insured Relapsing Multiple Sclerosis Patients Who Switched from Other Disease-Modifying Therapies to Teriflunomide, in the United States.\",\"authors\":\"Lita Araujo, Srikanth Kyatham, Kristen G Bzdek, Keiko Higuchi, Nupur Greene\",\"doi\":\"10.2147/CEOR.S401687\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Assess patient characteristics, healthcare resource utilization (HCRU), and relapses in patients with multiple sclerosis (MS) who switched to teriflunomide from other disease-modifying therapies (DMTs).</p><p><strong>Methods: </strong>Retrospective study of US Merative™ MarketScan<sup>®</sup> claims database (Jan 1, 2012-July 31, 2020,) including HIPAA-compliant, deidentified data. Patients ≥18 years with MS diagnosis (based on ICD-9/ICD-10 codes), receiving ≥1 DMT prior to teriflunomide and ≥12 months continuous enrollment pre and post index (date of teriflunomide initiation). Outcomes included inpatient and emergency room claims coinciding with MS diagnosis, MS-related healthcare costs, and annualized relapse rates (ARRs) (indirectly assessed using hospitalization/outpatient claims and steroid use coinciding with MS diagnosis).</p><p><strong>Results: </strong>The analyzed cohort (N=2016) was primarily female (79%); age (mean ± standard deviation) 51.4 ± 9.3 years; MS duration 4.7±2.8 years (at index). The majority (89.2%) were treated with one DMT before switching to teriflunomide. Use of outpatient services (event rate/100 person-years) increased post vs pre index; however, MRI visits significantly reduced over the same period (both <i>P</i><0.0001). Costs for MS-specific outpatient visits decreased by $371 per patient per year (PPPY) after switching to teriflunomide. Despite an increase in use post index (0.024 to 0.033 rate/100 person-years; <i>P</i><0.0001), costs for MS-specific laboratory services reduced (pre-index: $271 vs $248 PPPY post-index; <i>P</i>=0.02). Fewer patients had relapses after switching (pre-index: n=417 [20.7%]; post-index: n=333 [16.5%]). ARR was significantly lower after switching (pre-index: 0.269 vs post-index: 0.205; <i>P</i>=0.000).</p><p><strong>Conclusion: </strong>Switching to teriflunomide from existing DMTs in patients with relapsing MS resulted in a reduction in outpatient HCRU in this analysis of US claims data. The real-world effectiveness of teriflunomide was generally consistent with efficacy reported in clinical trials, showing a reduction in relapse following a switch to teriflunomide.</p>\",\"PeriodicalId\":47313,\"journal\":{\"name\":\"ClinicoEconomics and Outcomes Research\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e2/59/ceor-15-361.PMC10208242.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ClinicoEconomics and Outcomes Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/CEOR.S401687\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ClinicoEconomics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEOR.S401687","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Assessing the Health Economic Outcomes from Commercially Insured Relapsing Multiple Sclerosis Patients Who Switched from Other Disease-Modifying Therapies to Teriflunomide, in the United States.
Objective: Assess patient characteristics, healthcare resource utilization (HCRU), and relapses in patients with multiple sclerosis (MS) who switched to teriflunomide from other disease-modifying therapies (DMTs).
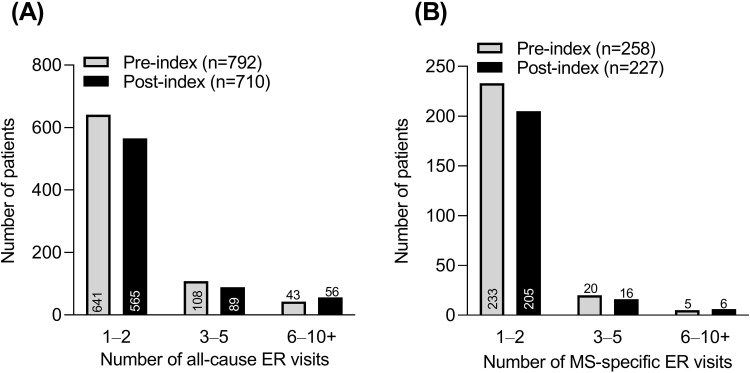
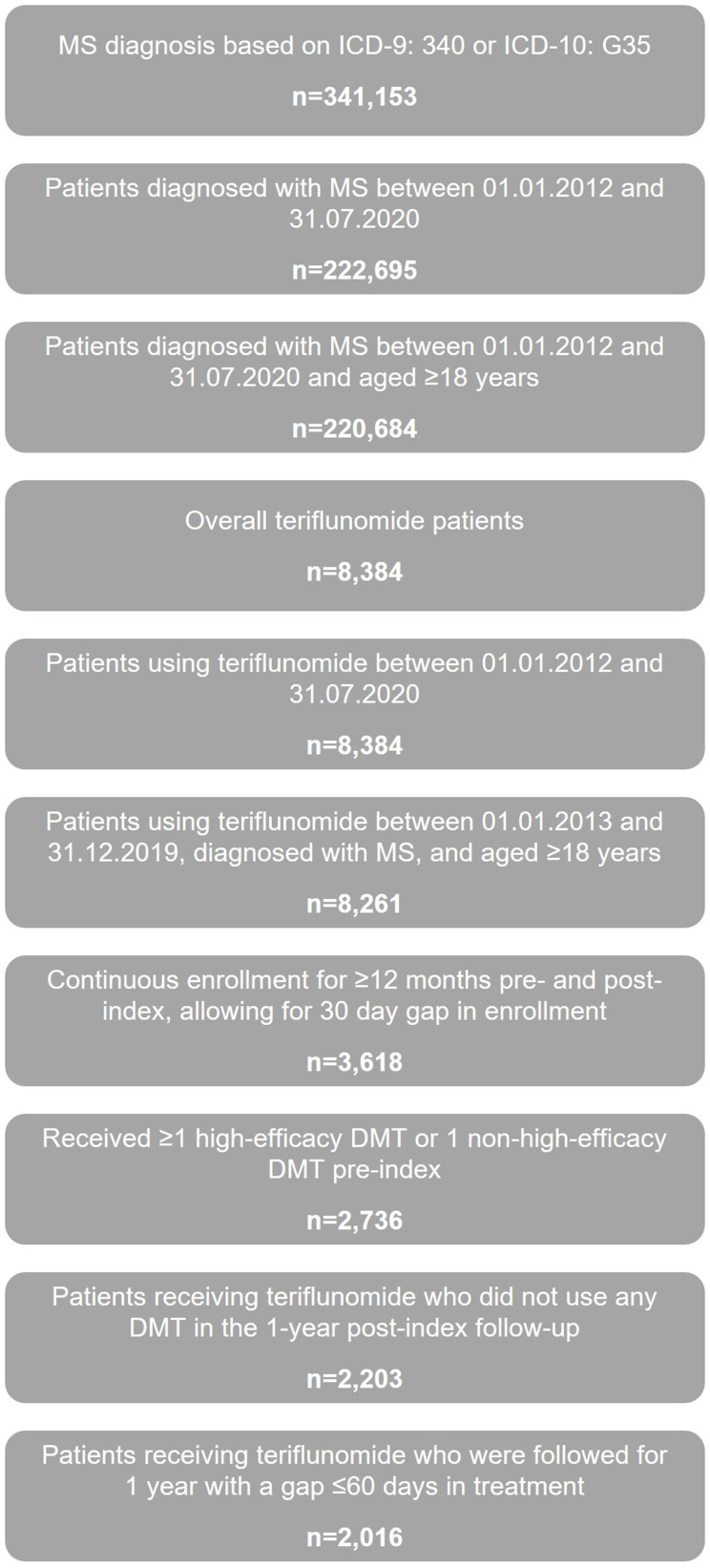
Methods: Retrospective study of US Merative™ MarketScan® claims database (Jan 1, 2012-July 31, 2020,) including HIPAA-compliant, deidentified data. Patients ≥18 years with MS diagnosis (based on ICD-9/ICD-10 codes), receiving ≥1 DMT prior to teriflunomide and ≥12 months continuous enrollment pre and post index (date of teriflunomide initiation). Outcomes included inpatient and emergency room claims coinciding with MS diagnosis, MS-related healthcare costs, and annualized relapse rates (ARRs) (indirectly assessed using hospitalization/outpatient claims and steroid use coinciding with MS diagnosis).
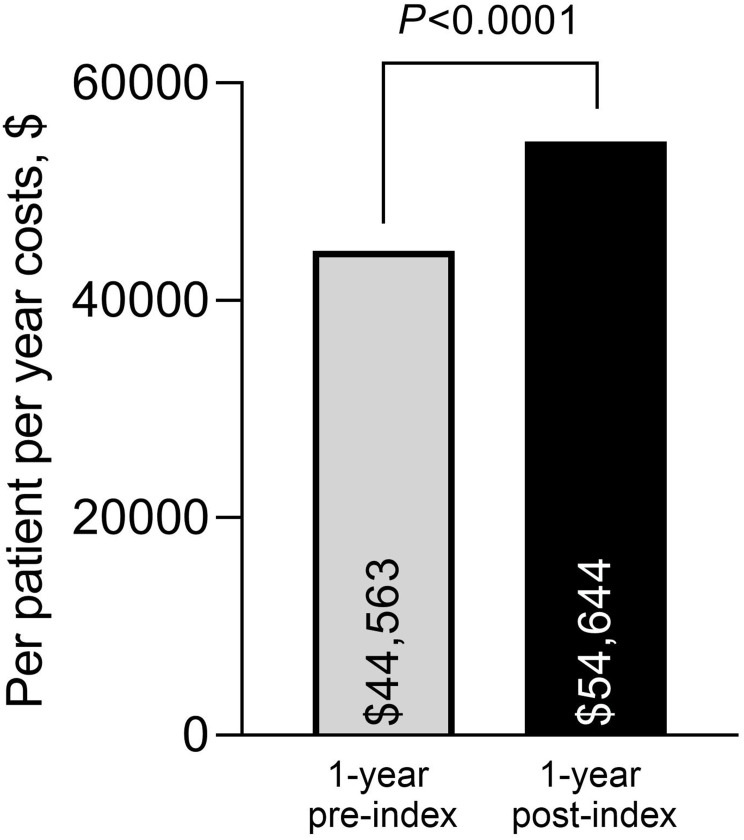
Results: The analyzed cohort (N=2016) was primarily female (79%); age (mean ± standard deviation) 51.4 ± 9.3 years; MS duration 4.7±2.8 years (at index). The majority (89.2%) were treated with one DMT before switching to teriflunomide. Use of outpatient services (event rate/100 person-years) increased post vs pre index; however, MRI visits significantly reduced over the same period (both P<0.0001). Costs for MS-specific outpatient visits decreased by $371 per patient per year (PPPY) after switching to teriflunomide. Despite an increase in use post index (0.024 to 0.033 rate/100 person-years; P<0.0001), costs for MS-specific laboratory services reduced (pre-index: $271 vs $248 PPPY post-index; P=0.02). Fewer patients had relapses after switching (pre-index: n=417 [20.7%]; post-index: n=333 [16.5%]). ARR was significantly lower after switching (pre-index: 0.269 vs post-index: 0.205; P=0.000).
Conclusion: Switching to teriflunomide from existing DMTs in patients with relapsing MS resulted in a reduction in outpatient HCRU in this analysis of US claims data. The real-world effectiveness of teriflunomide was generally consistent with efficacy reported in clinical trials, showing a reduction in relapse following a switch to teriflunomide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


