Ganga S Moorthy, Jordan S Pung, Neel Subramanian, B Jason Theiling, Emily C Sterrett
{"title":"医生分诊与改善儿科败血症护理之间的因果关系:单中心急诊科经验。","authors":"Ganga S Moorthy, Jordan S Pung, Neel Subramanian, B Jason Theiling, Emily C Sterrett","doi":"10.1097/pq9.0000000000000651","DOIUrl":null,"url":null,"abstract":"<p><p>Approximately 75,000 children are hospitalized for sepsis yearly in the United States, with 5%-20% mortality estimates. Outcomes are closely related to the timeliness of sepsis recognition and antibiotic administration.</p><p><strong>Methods: </strong>A multidisciplinary sepsis task force formed in the Spring of 2020 aimed to assess and improve pediatric sepsis care in the pediatric emergency department (ED). The electronic medical record identified pediatric sepsis patients from September 2015 to July 2021. Data for time to sepsis recognition and antibiotic delivery were analyzed using statistical process control charts (X̄-S charts). We identified special cause variation, and Bradford-Hill Criteria guided multidisciplinary discussions to identify the most probable cause.</p><p><strong>Results: </strong>In the fall of 2018, the average time from ED arrival to blood culture orders decreased by 1.1 hours, and the time from arrival to antibiotic administration decreased by 1.5 hours. After qualitative review, the task force hypothesized that initiation of attending-level pediatric physician-in-triage (P-PIT) as a part of ED triage was temporally associated with the observed improved sepsis care. P-PIT reduced the average time to the first provider exam by 14 minutes and introduced a process for physician evaluation before ED room assignment.</p><p><strong>Conclusions: </strong>Timely assessment by an attending-level physician improves time to sepsis recognition and antibiotic delivery in children who present to the ED with sepsis. Implementing a P-PIT program with early attending-level physician evaluation is a potential strategy for other institutions.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":null,"pages":null},"PeriodicalIF":1.2000,"publicationDate":"2023-05-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/97/20/pqs-8-e651.PMC10219727.pdf","citationCount":"0","resultStr":"{\"title\":\"Causal Association of Physician-in-Triage with Improved Pediatric Sepsis Care: A Single-Center, Emergency Department Experience.\",\"authors\":\"Ganga S Moorthy, Jordan S Pung, Neel Subramanian, B Jason Theiling, Emily C Sterrett\",\"doi\":\"10.1097/pq9.0000000000000651\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Approximately 75,000 children are hospitalized for sepsis yearly in the United States, with 5%-20% mortality estimates. Outcomes are closely related to the timeliness of sepsis recognition and antibiotic administration.</p><p><strong>Methods: </strong>A multidisciplinary sepsis task force formed in the Spring of 2020 aimed to assess and improve pediatric sepsis care in the pediatric emergency department (ED). The electronic medical record identified pediatric sepsis patients from September 2015 to July 2021. Data for time to sepsis recognition and antibiotic delivery were analyzed using statistical process control charts (X̄-S charts). We identified special cause variation, and Bradford-Hill Criteria guided multidisciplinary discussions to identify the most probable cause.</p><p><strong>Results: </strong>In the fall of 2018, the average time from ED arrival to blood culture orders decreased by 1.1 hours, and the time from arrival to antibiotic administration decreased by 1.5 hours. After qualitative review, the task force hypothesized that initiation of attending-level pediatric physician-in-triage (P-PIT) as a part of ED triage was temporally associated with the observed improved sepsis care. P-PIT reduced the average time to the first provider exam by 14 minutes and introduced a process for physician evaluation before ED room assignment.</p><p><strong>Conclusions: </strong>Timely assessment by an attending-level physician improves time to sepsis recognition and antibiotic delivery in children who present to the ED with sepsis. Implementing a P-PIT program with early attending-level physician evaluation is a potential strategy for other institutions.</p>\",\"PeriodicalId\":74412,\"journal\":{\"name\":\"Pediatric quality & safety\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2023-05-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/97/20/pqs-8-e651.PMC10219727.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric quality & safety\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/pq9.0000000000000651\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/5/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000651","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/5/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
Causal Association of Physician-in-Triage with Improved Pediatric Sepsis Care: A Single-Center, Emergency Department Experience.
Approximately 75,000 children are hospitalized for sepsis yearly in the United States, with 5%-20% mortality estimates. Outcomes are closely related to the timeliness of sepsis recognition and antibiotic administration.
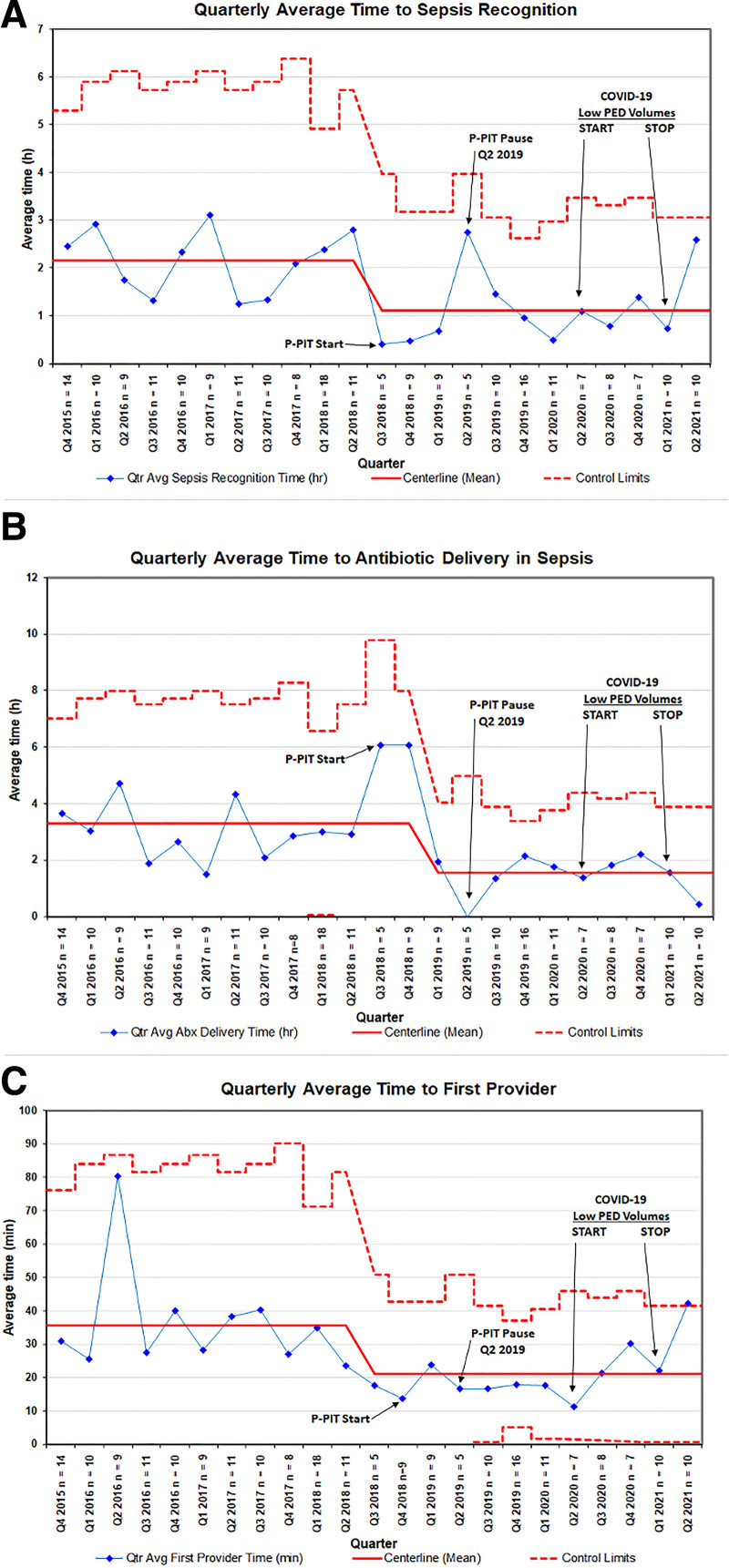
Methods: A multidisciplinary sepsis task force formed in the Spring of 2020 aimed to assess and improve pediatric sepsis care in the pediatric emergency department (ED). The electronic medical record identified pediatric sepsis patients from September 2015 to July 2021. Data for time to sepsis recognition and antibiotic delivery were analyzed using statistical process control charts (X̄-S charts). We identified special cause variation, and Bradford-Hill Criteria guided multidisciplinary discussions to identify the most probable cause.
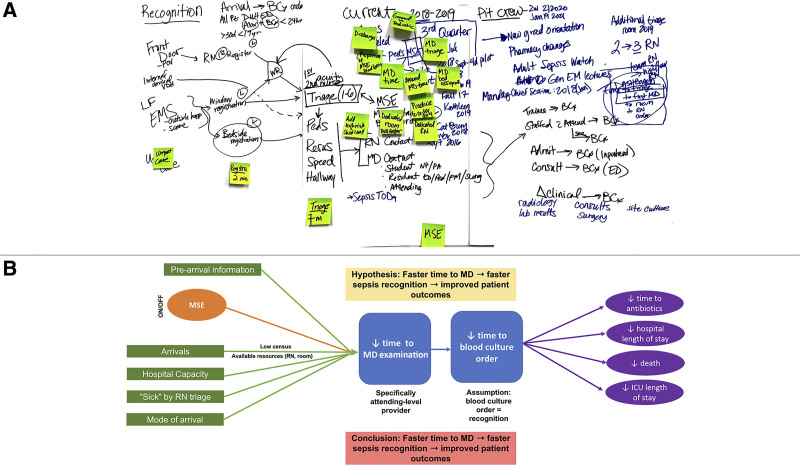
Results: In the fall of 2018, the average time from ED arrival to blood culture orders decreased by 1.1 hours, and the time from arrival to antibiotic administration decreased by 1.5 hours. After qualitative review, the task force hypothesized that initiation of attending-level pediatric physician-in-triage (P-PIT) as a part of ED triage was temporally associated with the observed improved sepsis care. P-PIT reduced the average time to the first provider exam by 14 minutes and introduced a process for physician evaluation before ED room assignment.
Conclusions: Timely assessment by an attending-level physician improves time to sepsis recognition and antibiotic delivery in children who present to the ED with sepsis. Implementing a P-PIT program with early attending-level physician evaluation is a potential strategy for other institutions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


