Muhammad Irfan Basheer, Iftikhar Ali Rana, Umer Nisar Sheikh, Muhammed Aasim Yusuf, Irfana Ishaq Sindhu, Asif Loya
{"title":"宪法不匹配修复缺陷综合征背景下急性淋巴母细胞淋巴瘤和结直肠癌的表现:一例病例报告并文献复习。","authors":"Muhammad Irfan Basheer, Iftikhar Ali Rana, Umer Nisar Sheikh, Muhammed Aasim Yusuf, Irfana Ishaq Sindhu, Asif Loya","doi":"10.37029/jcas.v8i1.443","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Constitutional mismatch repair deficiency (CMMRD) is a rare autosomal recessive disease carrying an increased risk of cancers (paediatric tumours of central nervous system, haematolymphoid malignancies along with gastrointestinal (GI) cancer(s), which are usually seen in the second and third decades), leading to syndromic presentation. Causal mutations are detected in DNA mismatch repair (MMR) genes, including MLH1, PMS2, MSH2 and MSH6 that are also known for their established role in Lynch syndrome. We describe a case of CMMRD with an earlier (first decade of life) presentation of mediastinal acute lymphoblastic lymphoma and colorectal malignancy.</p><p><strong>Case presentation: </strong>A 5-year-old boy presented with respiratory complaints, bilateral cervical lymphadenopathy, multiple café-au-lait macules (CALMs) on the lower back and history of parental consanguinity with the death of three sisters due to brain tumour within 6 months of diagnosis. Computerised tomographic scan chest revealed a huge mediastinal mass. The patient underwent a trucut biopsy of the mass. The results were significant for a pre-T-cell acute lymphoblastic lymphoma. Suspicion of CMMRD was raised based on a combination of factors described above. A panel of MMR proteins was applied on the biopsy tissue that revealed loss of nuclear expression of MLH1 and PMS2 immunostaining in tumour cells with positive external controls. While on maintenance therapy for lymphoma, about a year later, the patient developed subacute intestinal obstruction due to a stenosing polypoidal circumferential tumour in the mid-sigmoid colon found on flexible sigmoidoscopy that was followed by endoscopic biopsies and insertion of a fully covered self-expanding metallic adult biliary stent with a diameter of 10 mm and length of 6 cm leading to immediate relief of obstruction. Biopsies revealed adenocarcinoma with neuroendocrine differentiation. Metastatic tumour deposits were seen in the omentum, anterior abdominal wall and the left peritoneal wall.</p><p><strong>Practical implications: </strong>Earlier (first decade) presentation of GI malignancy warrants that an earlier screening through radiological scans for any possible tumours and MMR protein expression analysis (loss in tumour plus normal non-tumour cells) are essential in patients having CALMs and family history of paediatric tumours.</p>","PeriodicalId":73631,"journal":{"name":"Journal of cancer & allied specialties","volume":"8 1","pages":"e443"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/de/02/JCAS-8-443.PMC10166326.pdf","citationCount":"0","resultStr":"{\"title\":\"Presentation of Acute Lymphoblastic Lymphoma and Colorectal Carcinoma in the Context of Constitutional Mismatch Repair Deficiency Syndrome: A Case Report with Literature Review.\",\"authors\":\"Muhammad Irfan Basheer, Iftikhar Ali Rana, Umer Nisar Sheikh, Muhammed Aasim Yusuf, Irfana Ishaq Sindhu, Asif Loya\",\"doi\":\"10.37029/jcas.v8i1.443\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Constitutional mismatch repair deficiency (CMMRD) is a rare autosomal recessive disease carrying an increased risk of cancers (paediatric tumours of central nervous system, haematolymphoid malignancies along with gastrointestinal (GI) cancer(s), which are usually seen in the second and third decades), leading to syndromic presentation. Causal mutations are detected in DNA mismatch repair (MMR) genes, including MLH1, PMS2, MSH2 and MSH6 that are also known for their established role in Lynch syndrome. We describe a case of CMMRD with an earlier (first decade of life) presentation of mediastinal acute lymphoblastic lymphoma and colorectal malignancy.</p><p><strong>Case presentation: </strong>A 5-year-old boy presented with respiratory complaints, bilateral cervical lymphadenopathy, multiple café-au-lait macules (CALMs) on the lower back and history of parental consanguinity with the death of three sisters due to brain tumour within 6 months of diagnosis. Computerised tomographic scan chest revealed a huge mediastinal mass. The patient underwent a trucut biopsy of the mass. The results were significant for a pre-T-cell acute lymphoblastic lymphoma. Suspicion of CMMRD was raised based on a combination of factors described above. A panel of MMR proteins was applied on the biopsy tissue that revealed loss of nuclear expression of MLH1 and PMS2 immunostaining in tumour cells with positive external controls. While on maintenance therapy for lymphoma, about a year later, the patient developed subacute intestinal obstruction due to a stenosing polypoidal circumferential tumour in the mid-sigmoid colon found on flexible sigmoidoscopy that was followed by endoscopic biopsies and insertion of a fully covered self-expanding metallic adult biliary stent with a diameter of 10 mm and length of 6 cm leading to immediate relief of obstruction. Biopsies revealed adenocarcinoma with neuroendocrine differentiation. Metastatic tumour deposits were seen in the omentum, anterior abdominal wall and the left peritoneal wall.</p><p><strong>Practical implications: </strong>Earlier (first decade) presentation of GI malignancy warrants that an earlier screening through radiological scans for any possible tumours and MMR protein expression analysis (loss in tumour plus normal non-tumour cells) are essential in patients having CALMs and family history of paediatric tumours.</p>\",\"PeriodicalId\":73631,\"journal\":{\"name\":\"Journal of cancer & allied specialties\",\"volume\":\"8 1\",\"pages\":\"e443\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-01-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/de/02/JCAS-8-443.PMC10166326.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of cancer & allied specialties\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.37029/jcas.v8i1.443\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cancer & allied specialties","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.37029/jcas.v8i1.443","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Presentation of Acute Lymphoblastic Lymphoma and Colorectal Carcinoma in the Context of Constitutional Mismatch Repair Deficiency Syndrome: A Case Report with Literature Review.
Introduction: Constitutional mismatch repair deficiency (CMMRD) is a rare autosomal recessive disease carrying an increased risk of cancers (paediatric tumours of central nervous system, haematolymphoid malignancies along with gastrointestinal (GI) cancer(s), which are usually seen in the second and third decades), leading to syndromic presentation. Causal mutations are detected in DNA mismatch repair (MMR) genes, including MLH1, PMS2, MSH2 and MSH6 that are also known for their established role in Lynch syndrome. We describe a case of CMMRD with an earlier (first decade of life) presentation of mediastinal acute lymphoblastic lymphoma and colorectal malignancy.
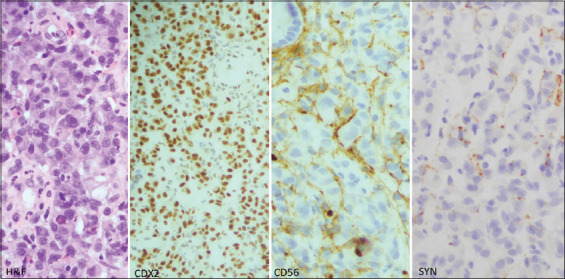
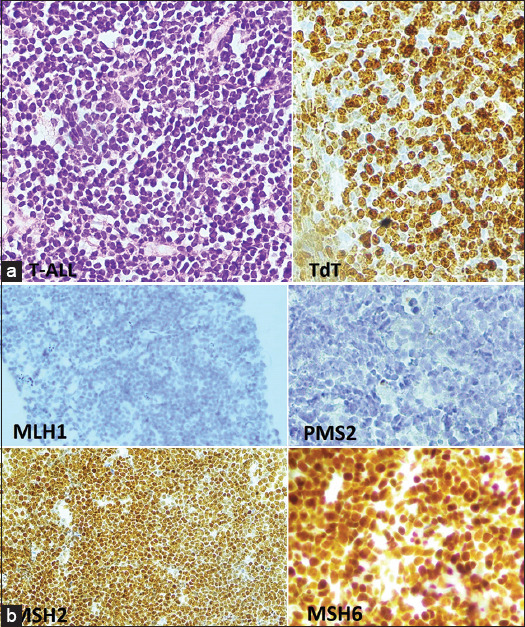
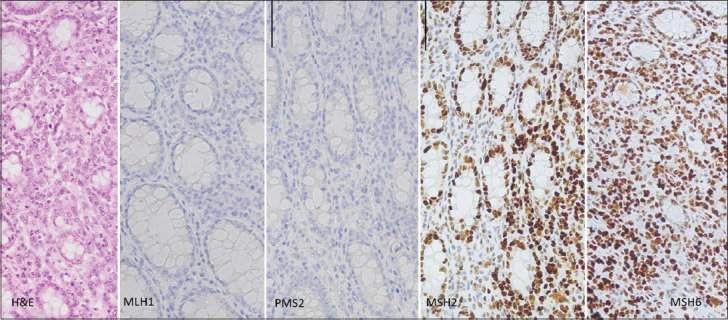
Case presentation: A 5-year-old boy presented with respiratory complaints, bilateral cervical lymphadenopathy, multiple café-au-lait macules (CALMs) on the lower back and history of parental consanguinity with the death of three sisters due to brain tumour within 6 months of diagnosis. Computerised tomographic scan chest revealed a huge mediastinal mass. The patient underwent a trucut biopsy of the mass. The results were significant for a pre-T-cell acute lymphoblastic lymphoma. Suspicion of CMMRD was raised based on a combination of factors described above. A panel of MMR proteins was applied on the biopsy tissue that revealed loss of nuclear expression of MLH1 and PMS2 immunostaining in tumour cells with positive external controls. While on maintenance therapy for lymphoma, about a year later, the patient developed subacute intestinal obstruction due to a stenosing polypoidal circumferential tumour in the mid-sigmoid colon found on flexible sigmoidoscopy that was followed by endoscopic biopsies and insertion of a fully covered self-expanding metallic adult biliary stent with a diameter of 10 mm and length of 6 cm leading to immediate relief of obstruction. Biopsies revealed adenocarcinoma with neuroendocrine differentiation. Metastatic tumour deposits were seen in the omentum, anterior abdominal wall and the left peritoneal wall.
Practical implications: Earlier (first decade) presentation of GI malignancy warrants that an earlier screening through radiological scans for any possible tumours and MMR protein expression analysis (loss in tumour plus normal non-tumour cells) are essential in patients having CALMs and family history of paediatric tumours.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


