{"title":"退行性腰椎疾病患者斜位腰椎融合术后椎间盘突出引起的对侧下肢神经根病:例证性病例。","authors":"Satoshi Hattori, Toru Maeda","doi":"10.3171/CASE23198","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Contralateral lower limb radiculopathy is a potential early complication of oblique lumbar interbody fusion (OLIF) in degenerative lumbar disorders. Among several pathologies related to contralateral radiculopathy following OLIF, extraforaminal disc herniation during the OLIF procedure is very rare.</p><p><strong>Observations: </strong>Case 1 is a 68-year-old male underwent L4-5 and L5-6 OLIF for recurrent lumbar canal stenosis-expressed right leg pain and muscle weakness after surgery. Case 2 is a 76-year-old female on whom L4-5 OLIF was performed for L4 degenerative spondylolisthesis and who presented right leg pain and numbness postoperatively. In both patients, OLIF cages were inserted into the posterior part of the disc space or obliquely and the extraforaminal extruded disc compressed opposite exiting nerve roots (L5 root in case 1 and L4 root in case 2) as shown on magnetic resonance imaging (MRI). Surgical decompression with discectomy was required for pain relief and neurological improvement in both cases.</p><p><strong>Lessons: </strong>When emerging from new-onset opposite limb radiculopathy attributed to the OLIF procedure, extraforaminal disc herniation should be considered a potential pathology and MRI is useful for early diagnosis and selecting a subsequent management, including surgery.</p>","PeriodicalId":16554,"journal":{"name":"Journal of Neurosurgery: Case Lessons","volume":"5 22","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-05-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/17/7e/CASE23198.PMC10550671.pdf","citationCount":"0","resultStr":"{\"title\":\"Contralateral lower limb radiculopathy by extraforaminal disc herniation following oblique lumbar interbody fusion in degenerative lumbar disorder: illustrative cases.\",\"authors\":\"Satoshi Hattori, Toru Maeda\",\"doi\":\"10.3171/CASE23198\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Contralateral lower limb radiculopathy is a potential early complication of oblique lumbar interbody fusion (OLIF) in degenerative lumbar disorders. Among several pathologies related to contralateral radiculopathy following OLIF, extraforaminal disc herniation during the OLIF procedure is very rare.</p><p><strong>Observations: </strong>Case 1 is a 68-year-old male underwent L4-5 and L5-6 OLIF for recurrent lumbar canal stenosis-expressed right leg pain and muscle weakness after surgery. Case 2 is a 76-year-old female on whom L4-5 OLIF was performed for L4 degenerative spondylolisthesis and who presented right leg pain and numbness postoperatively. In both patients, OLIF cages were inserted into the posterior part of the disc space or obliquely and the extraforaminal extruded disc compressed opposite exiting nerve roots (L5 root in case 1 and L4 root in case 2) as shown on magnetic resonance imaging (MRI). Surgical decompression with discectomy was required for pain relief and neurological improvement in both cases.</p><p><strong>Lessons: </strong>When emerging from new-onset opposite limb radiculopathy attributed to the OLIF procedure, extraforaminal disc herniation should be considered a potential pathology and MRI is useful for early diagnosis and selecting a subsequent management, including surgery.</p>\",\"PeriodicalId\":16554,\"journal\":{\"name\":\"Journal of Neurosurgery: Case Lessons\",\"volume\":\"5 22\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-05-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/17/7e/CASE23198.PMC10550671.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Neurosurgery: Case Lessons\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3171/CASE23198\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neurosurgery: Case Lessons","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3171/CASE23198","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Contralateral lower limb radiculopathy by extraforaminal disc herniation following oblique lumbar interbody fusion in degenerative lumbar disorder: illustrative cases.
Background: Contralateral lower limb radiculopathy is a potential early complication of oblique lumbar interbody fusion (OLIF) in degenerative lumbar disorders. Among several pathologies related to contralateral radiculopathy following OLIF, extraforaminal disc herniation during the OLIF procedure is very rare.
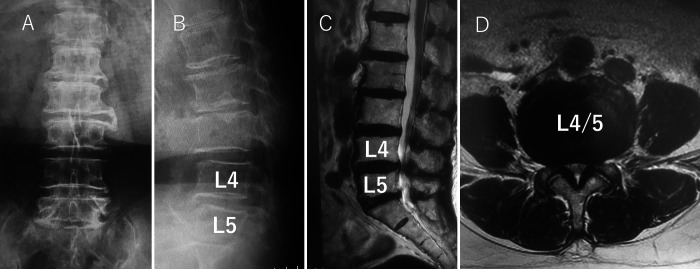
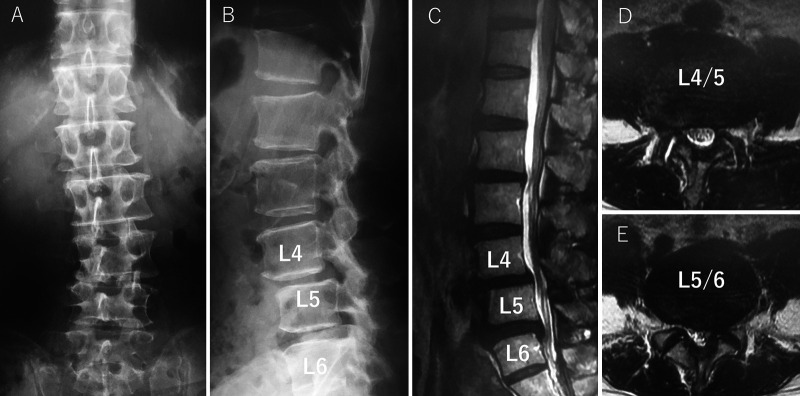
Observations: Case 1 is a 68-year-old male underwent L4-5 and L5-6 OLIF for recurrent lumbar canal stenosis-expressed right leg pain and muscle weakness after surgery. Case 2 is a 76-year-old female on whom L4-5 OLIF was performed for L4 degenerative spondylolisthesis and who presented right leg pain and numbness postoperatively. In both patients, OLIF cages were inserted into the posterior part of the disc space or obliquely and the extraforaminal extruded disc compressed opposite exiting nerve roots (L5 root in case 1 and L4 root in case 2) as shown on magnetic resonance imaging (MRI). Surgical decompression with discectomy was required for pain relief and neurological improvement in both cases.
Lessons: When emerging from new-onset opposite limb radiculopathy attributed to the OLIF procedure, extraforaminal disc herniation should be considered a potential pathology and MRI is useful for early diagnosis and selecting a subsequent management, including surgery.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


