Angelo V Vasiliadis, Timothy Lording, Robin Canetti, Elvire Servien, Sébastien Lustig, Cécile Batailler
{"title":"在全膝关节置换术中,我们多久需要一次矫正柄?大约连续789个膝盖。","authors":"Angelo V Vasiliadis, Timothy Lording, Robin Canetti, Elvire Servien, Sébastien Lustig, Cécile Batailler","doi":"10.1051/sicotj/2023012","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>This study aimed to determine the incidence of offset stem usage in revision total knee arthroplasty (rTKA), and to assess the necessity for their use with the femoral and tibial components.</p><p><strong>Methods: </strong>This retrospective radiological study included 862 patients who underwent rTKA between 2010 and 2022. Patients were divided into a non-stem group (group NS), offset stem group (group OS), and straight stem group (group SS). Two senior orthopedic surgeons evaluated all the post-operative radiographs of the group OS to assess the necessity of offset use.</p><p><strong>Results: </strong>In total, 789 patients met all eligibility inclusion criteria and were reviewed (305 males (38.7%)) with a mean age of 72.7 ± 10.2 years old [39; 96]. Eighty-eight (11.1%) patients had undergone rTKA with offset stems (34 tibia, 31 femur, 24 both) and 609 (70.2%) with straight stems. The tibial and femoral stems were diaphyseal of over 75 mm in 83 revisions (94.3%) for group OS and 444 revisions (72.9%) for group SS (p < 0.001). Offset in the tibial component was located medially in 50% of rTKA, while the offset in the femoral component was placed anteriorly in 47.3% of the rTKA. Assessment by the two independent senior surgeons found stems were only necessary in 3.4% of cases. Offset stems were only required for the tibial implant.</p><p><strong>Discussion: </strong>Offset stems were used in 11.1% of revision total knee replacements, however, they were deemed necessary in 3.4% and for the tibial component only.</p>","PeriodicalId":46378,"journal":{"name":"SICOT-J","volume":"9 ","pages":"15"},"PeriodicalIF":1.8000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10226448/pdf/","citationCount":"0","resultStr":"{\"title\":\"How often do we need offset stems for revision total knee arthroplasty? About a consecutive series of 789 knees.\",\"authors\":\"Angelo V Vasiliadis, Timothy Lording, Robin Canetti, Elvire Servien, Sébastien Lustig, Cécile Batailler\",\"doi\":\"10.1051/sicotj/2023012\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>This study aimed to determine the incidence of offset stem usage in revision total knee arthroplasty (rTKA), and to assess the necessity for their use with the femoral and tibial components.</p><p><strong>Methods: </strong>This retrospective radiological study included 862 patients who underwent rTKA between 2010 and 2022. Patients were divided into a non-stem group (group NS), offset stem group (group OS), and straight stem group (group SS). Two senior orthopedic surgeons evaluated all the post-operative radiographs of the group OS to assess the necessity of offset use.</p><p><strong>Results: </strong>In total, 789 patients met all eligibility inclusion criteria and were reviewed (305 males (38.7%)) with a mean age of 72.7 ± 10.2 years old [39; 96]. Eighty-eight (11.1%) patients had undergone rTKA with offset stems (34 tibia, 31 femur, 24 both) and 609 (70.2%) with straight stems. The tibial and femoral stems were diaphyseal of over 75 mm in 83 revisions (94.3%) for group OS and 444 revisions (72.9%) for group SS (p < 0.001). Offset in the tibial component was located medially in 50% of rTKA, while the offset in the femoral component was placed anteriorly in 47.3% of the rTKA. Assessment by the two independent senior surgeons found stems were only necessary in 3.4% of cases. Offset stems were only required for the tibial implant.</p><p><strong>Discussion: </strong>Offset stems were used in 11.1% of revision total knee replacements, however, they were deemed necessary in 3.4% and for the tibial component only.</p>\",\"PeriodicalId\":46378,\"journal\":{\"name\":\"SICOT-J\",\"volume\":\"9 \",\"pages\":\"15\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10226448/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"SICOT-J\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1051/sicotj/2023012\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"SICOT-J","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1051/sicotj/2023012","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
How often do we need offset stems for revision total knee arthroplasty? About a consecutive series of 789 knees.
Introduction: This study aimed to determine the incidence of offset stem usage in revision total knee arthroplasty (rTKA), and to assess the necessity for their use with the femoral and tibial components.
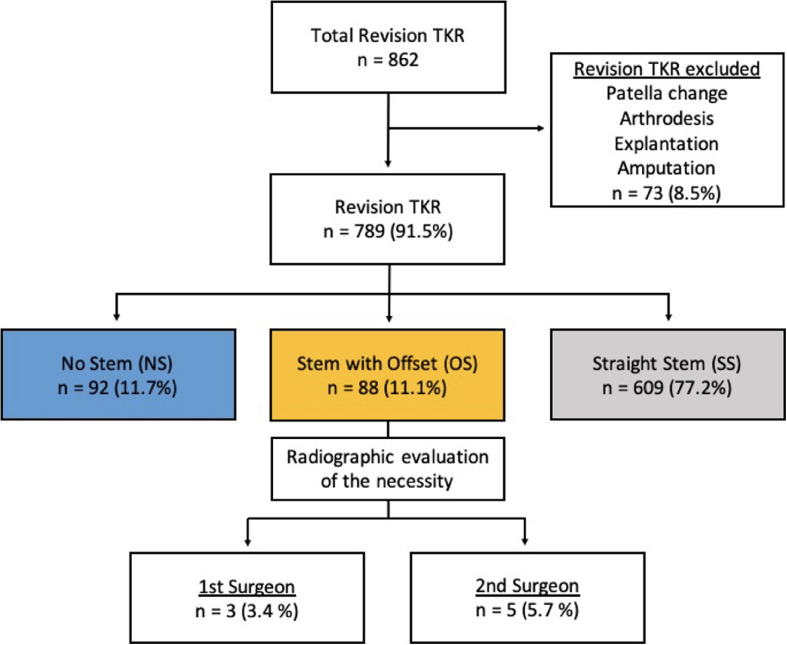
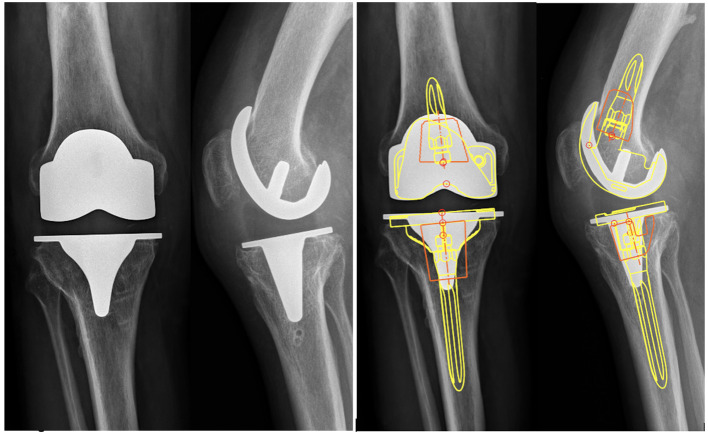
Methods: This retrospective radiological study included 862 patients who underwent rTKA between 2010 and 2022. Patients were divided into a non-stem group (group NS), offset stem group (group OS), and straight stem group (group SS). Two senior orthopedic surgeons evaluated all the post-operative radiographs of the group OS to assess the necessity of offset use.
Results: In total, 789 patients met all eligibility inclusion criteria and were reviewed (305 males (38.7%)) with a mean age of 72.7 ± 10.2 years old [39; 96]. Eighty-eight (11.1%) patients had undergone rTKA with offset stems (34 tibia, 31 femur, 24 both) and 609 (70.2%) with straight stems. The tibial and femoral stems were diaphyseal of over 75 mm in 83 revisions (94.3%) for group OS and 444 revisions (72.9%) for group SS (p < 0.001). Offset in the tibial component was located medially in 50% of rTKA, while the offset in the femoral component was placed anteriorly in 47.3% of the rTKA. Assessment by the two independent senior surgeons found stems were only necessary in 3.4% of cases. Offset stems were only required for the tibial implant.
Discussion: Offset stems were used in 11.1% of revision total knee replacements, however, they were deemed necessary in 3.4% and for the tibial component only.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


