Jason W. Greenberg MD, Muhammad Aanish Raees MBBS, Alia Dani MD, MPH, Haleh C. Heydarian MD, Clifford Chin MD, Farhan Zafar MD, MS, David G. Lehenbauer MD, David L.S. Morales MD
{"title":"与非单心室先天性心脏病患者相比,缓和型左心室发育不全综合征患者的候诊时间更长,心脏移植后存活率相当。","authors":"Jason W. Greenberg MD, Muhammad Aanish Raees MBBS, Alia Dani MD, MPH, Haleh C. Heydarian MD, Clifford Chin MD, Farhan Zafar MD, MS, David G. Lehenbauer MD, David L.S. Morales MD","doi":"10.1053/j.semtcvs.2022.08.019","DOIUrl":null,"url":null,"abstract":"<div><p><span><span>Congenital heart disease (CHD) is a well-established risk factor for inferior waitlist and post-heart </span>transplant survival<span><span><span> in children. Differences in outcomes between CHD subgroups are understudied. The present study compared outcomes for palliated hypoplastic left heart syndrome (HLHS) patients to other non-single ventricle CHD (non-SVCHD) and non-CHD patients. United Network for Organ Sharing was used to identify children (age < 18) listed for </span>heart transplant in the United States between 2016 and 2021. CHD sub-diagnoses were only available for United Network for Organ Sharing status 1a after 2015, thereby defining the cohort. Waitlist outcomes were studied using competing-risk time-to-event analysis for transplantation, mortality/decompensation, and alive-on-waitlist. Multivariable Cox </span>proportional hazards regression analyses were used to identify factors associated with inferior post-transplant survival. Patients included: palliated-HLHS (</span></span><em>n =</em> 477), non-SVCHD (<em>n =</em> 686), and non-CHD (<em>n =</em> 1261). At listing, Palliated-HLHS patients were older than non-SVCHD (median 2-year [IQR 0-8] vs median 0-year [0-3], respectively) and younger than non-CHD (median 7-year [0-14]) (<em>P <</em> 0.001 vs both), and were more likely to be white (<em>P <</em> 0.01 vs both). Upon time-to-event analysis, rates of waitlist mortality/decompensation rates were greater among non-SVCHD than palliated-HLHS. Post-transplant survival was comparable between palliated-HLHS and non-SVCHD (<em>P =</em> 0.920) but worse compared to non-CHD (<em>P <</em> 0.001). Both palliated-HLHS (HR 2.40 [95% CI 1.68-3.42]) and non-SVSCHD (2.04 [1.39-2.99]) were independently associated with post-transplant mortality. Palliated-HLHS patients with heart failure experience significantly worse post-transplant outcomes than non-CHD but, compared to other CHD patients, experience superior waitlist and comparable post-transplant survival. While a high-risk cohort, HLHS patients can achieve gratifying waitlist and post-transplant survival.</p></div>","PeriodicalId":48592,"journal":{"name":"Seminars in Thoracic and Cardiovascular Surgery","volume":"36 2","pages":"Pages 230-241"},"PeriodicalIF":2.5000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Palliated Hypoplastic Left Heart Syndrome Patients Experience Superior Waitlist and Comparable Post-Heart Transplant Survival to Non-Single Ventricle Congenital Heart Disease Patients\",\"authors\":\"Jason W. Greenberg MD, Muhammad Aanish Raees MBBS, Alia Dani MD, MPH, Haleh C. Heydarian MD, Clifford Chin MD, Farhan Zafar MD, MS, David G. Lehenbauer MD, David L.S. Morales MD\",\"doi\":\"10.1053/j.semtcvs.2022.08.019\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><p><span><span>Congenital heart disease (CHD) is a well-established risk factor for inferior waitlist and post-heart </span>transplant survival<span><span><span> in children. Differences in outcomes between CHD subgroups are understudied. The present study compared outcomes for palliated hypoplastic left heart syndrome (HLHS) patients to other non-single ventricle CHD (non-SVCHD) and non-CHD patients. United Network for Organ Sharing was used to identify children (age < 18) listed for </span>heart transplant in the United States between 2016 and 2021. CHD sub-diagnoses were only available for United Network for Organ Sharing status 1a after 2015, thereby defining the cohort. Waitlist outcomes were studied using competing-risk time-to-event analysis for transplantation, mortality/decompensation, and alive-on-waitlist. Multivariable Cox </span>proportional hazards regression analyses were used to identify factors associated with inferior post-transplant survival. Patients included: palliated-HLHS (</span></span><em>n =</em> 477), non-SVCHD (<em>n =</em> 686), and non-CHD (<em>n =</em> 1261). At listing, Palliated-HLHS patients were older than non-SVCHD (median 2-year [IQR 0-8] vs median 0-year [0-3], respectively) and younger than non-CHD (median 7-year [0-14]) (<em>P <</em> 0.001 vs both), and were more likely to be white (<em>P <</em> 0.01 vs both). Upon time-to-event analysis, rates of waitlist mortality/decompensation rates were greater among non-SVCHD than palliated-HLHS. Post-transplant survival was comparable between palliated-HLHS and non-SVCHD (<em>P =</em> 0.920) but worse compared to non-CHD (<em>P <</em> 0.001). Both palliated-HLHS (HR 2.40 [95% CI 1.68-3.42]) and non-SVSCHD (2.04 [1.39-2.99]) were independently associated with post-transplant mortality. Palliated-HLHS patients with heart failure experience significantly worse post-transplant outcomes than non-CHD but, compared to other CHD patients, experience superior waitlist and comparable post-transplant survival. While a high-risk cohort, HLHS patients can achieve gratifying waitlist and post-transplant survival.</p></div>\",\"PeriodicalId\":48592,\"journal\":{\"name\":\"Seminars in Thoracic and Cardiovascular Surgery\",\"volume\":\"36 2\",\"pages\":\"Pages 230-241\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Seminars in Thoracic and Cardiovascular Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S1043067922002714\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Seminars in Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1043067922002714","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
先天性心脏病(CHD)是导致儿童等待心脏移植和移植后存活率较低的一个公认的风险因素。对先天性心脏病亚组之间的预后差异研究不足。本研究将缓和型左心发育不全综合征(HLHS)患者的预后与其他非单室先天性心脏病(non-SVCHD)和非先天性心脏病患者的预后进行了比较。研究使用器官共享联合网络(United Network for Organ Sharing)来识别2016年至2021年期间在美国被列入心脏移植名单的儿童(年龄小于18岁)。只有在 2015 年之后,器官共享联合网络状态 1a 的 CHD 子诊断才可用,从而确定了队列。采用竞争风险时间到事件分析法研究了移植、死亡率/代偿率和候诊存活率的候诊结果。多变量考克斯比例危险回归分析用于确定与移植后存活率较低相关的因素。患者包括:缓和-HLHS(n = 477)、非 SVCHD(n = 686)和非CHD(n = 1261)。入院时,Palliated-HLHS 患者的年龄比非 SVCHD 患者大(中位数分别为 2 年 [IQR 0-8] vs 中位数 0 年 [0-3]),比非CHD 患者年轻(中位数为 7 年 [0-14] )(P < 0.001 vs 两者),更可能是白人(P < 0.01 vs 两者)。从时间到事件的分析来看,非 SVCHD 患者的候诊死亡率/代偿率高于缓和型 HLHS 患者。经姑息治疗的慢性阻塞性肺疾病患者与非慢性阻塞性肺疾病患者的移植后存活率相当(P = 0.920),但与非慢性阻塞性肺疾病患者相比更差(P < 0.001)。姑息-HLHS(HR 2.40 [95% CI 1.68-3.42])和非 SVSCHD(2.04 [1.39-2.99])均与移植后死亡率独立相关。患有心力衰竭的缓和型 HLHS 患者移植后的预后明显差于非心脏病患者,但与其他心脏病患者相比,他们的候选生存率更高,移植后生存率也相当。虽然HLHS患者属于高危人群,但他们在等待移植和移植后的存活率方面都令人满意。
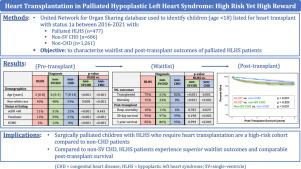
Palliated Hypoplastic Left Heart Syndrome Patients Experience Superior Waitlist and Comparable Post-Heart Transplant Survival to Non-Single Ventricle Congenital Heart Disease Patients
Congenital heart disease (CHD) is a well-established risk factor for inferior waitlist and post-heart transplant survival in children. Differences in outcomes between CHD subgroups are understudied. The present study compared outcomes for palliated hypoplastic left heart syndrome (HLHS) patients to other non-single ventricle CHD (non-SVCHD) and non-CHD patients. United Network for Organ Sharing was used to identify children (age < 18) listed for heart transplant in the United States between 2016 and 2021. CHD sub-diagnoses were only available for United Network for Organ Sharing status 1a after 2015, thereby defining the cohort. Waitlist outcomes were studied using competing-risk time-to-event analysis for transplantation, mortality/decompensation, and alive-on-waitlist. Multivariable Cox proportional hazards regression analyses were used to identify factors associated with inferior post-transplant survival. Patients included: palliated-HLHS (n = 477), non-SVCHD (n = 686), and non-CHD (n = 1261). At listing, Palliated-HLHS patients were older than non-SVCHD (median 2-year [IQR 0-8] vs median 0-year [0-3], respectively) and younger than non-CHD (median 7-year [0-14]) (P < 0.001 vs both), and were more likely to be white (P < 0.01 vs both). Upon time-to-event analysis, rates of waitlist mortality/decompensation rates were greater among non-SVCHD than palliated-HLHS. Post-transplant survival was comparable between palliated-HLHS and non-SVCHD (P = 0.920) but worse compared to non-CHD (P < 0.001). Both palliated-HLHS (HR 2.40 [95% CI 1.68-3.42]) and non-SVSCHD (2.04 [1.39-2.99]) were independently associated with post-transplant mortality. Palliated-HLHS patients with heart failure experience significantly worse post-transplant outcomes than non-CHD but, compared to other CHD patients, experience superior waitlist and comparable post-transplant survival. While a high-risk cohort, HLHS patients can achieve gratifying waitlist and post-transplant survival.
期刊介绍:
Seminars in Thoracic and Cardiovascular Surgery is devoted to providing a forum for cardiothoracic surgeons to disseminate and discuss important new information and to gain insight into unresolved areas of question in the specialty. Each issue presents readers with a selection of original peer-reviewed articles accompanied by editorial commentary from specialists in the field. In addition, readers are offered valuable invited articles: State of Views editorials and Current Readings highlighting the latest contributions on central or controversial issues. Another prized feature is expert roundtable discussions in which experts debate critical questions for cardiothoracic treatment and care. Seminars is an invitation-only publication that receives original submissions transferred ONLY from its sister publication, The Journal of Thoracic and Cardiovascular Surgery. As we continue to expand the reach of the Journal, we will explore the possibility of accepting unsolicited manuscripts in the future.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


