{"title":"分析尿C-C基序趋化因子配体14 (CCL14)和第一代尿生物标志物预测急性肾损伤后肾脏恢复:一项前瞻性探索性研究。","authors":"Ben-Shu Qian, Hui-Miao Jia, Yi-Bing Weng, Xin-Cheng Li, Chao-Dong Chen, Fang-Xing Guo, Yu-Zhen Han, Li-Feng Huang, Yue Zheng, Wen-Xiong Li","doi":"10.1186/s40560-023-00659-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute kidney injury (AKI) is a frequent syndrome in the intensive care unit (ICU). AKI patients with kidney function recovery have better short-term and long-term prognoses compared with those with non-recovery. Numerous studies focus on biomarkers to distinguish them. To better understand the predictive performance of urinary biomarkers of renal recovery in patients with AKI, we evaluated C-C motif chemokine ligand 14 (CCL14) and two first-generation biomarkers (cell cycle arrest biomarkers and neutrophil gelatinase-associated lipocalin) in two ICU settings.</p><p><strong>Methods: </strong>We performed a prospective study to analyze urinary biomarkers for predicting renal recovery from AKI. Patients who developed AKI after ICU admission were enrolled and urinary biomarkers including tissue inhibitor of metalloproteinase-2 (TIMP-2), insulin-like growth factor-binding protein 7 (IGFBP7), CCL14, and neutrophil gelatinase-associated lipocalin (NGAL) were detected on the day of AKI diagnosis. The primary endpoint was non-recovery from AKI within 7 days. The individual discriminative ability of CCL14, [TIMP-2] × [IGFBP7] and NGAL to predict renal non-recovery were evaluated by the area under receiver operating characteristics curve (AUC).</p><p><strong>Results: </strong>Of 164 AKI patients, 64 (39.0%) failed to recover from AKI onset. CCL14 showed a fair prediction ability for renal non-recovery with an AUC of 0.71 (95% CI 0.63-0.77, p < 0.001). [TIMP-2] × [IGFBP7] showed the best prediction for renal non-recovery with an AUC of 0.78 (95% CI 0.71-0.84, p < 0.001). However, NGAL had no use in predicting non-recovery with an AUC of 0.53 (95% CI 0.45-0.60, p = 0.562). A two-parameter model (non-renal SOFA score and AKI stage) predicted renal non-recovery with an AUC of 0.77 (95% CI 0.77-0.83, p = 0.004). When [TIMP-2] × [IGFBP7] was combined with the clinical factors, the AUC was significantly improved to 0.82 (95% CI 0.74-0.87, p = 0.049).</p><p><strong>Conclusions: </strong>Urinary CCL14 and [TIMP-2] × [IGFBP7] were fair predictors of renal non-recovery from AKI. Combing urinary [TIMP-2] × [IGFBP7] with a clinical model consisting of non-renal SOFA score and AKI stage enhanced the predictive power for renal non-recovery. Urinary CCL14 showed no significant advantage in predicting renal non-recovery compared to [TIMP-2] × [IGFBP7].</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":"11 1","pages":"11"},"PeriodicalIF":3.8000,"publicationDate":"2023-03-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10026399/pdf/","citationCount":"2","resultStr":"{\"title\":\"Analysis of urinary C-C motif chemokine ligand 14 (CCL14) and first-generation urinary biomarkers for predicting renal recovery from acute kidney injury: a prospective exploratory study.\",\"authors\":\"Ben-Shu Qian, Hui-Miao Jia, Yi-Bing Weng, Xin-Cheng Li, Chao-Dong Chen, Fang-Xing Guo, Yu-Zhen Han, Li-Feng Huang, Yue Zheng, Wen-Xiong Li\",\"doi\":\"10.1186/s40560-023-00659-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Acute kidney injury (AKI) is a frequent syndrome in the intensive care unit (ICU). AKI patients with kidney function recovery have better short-term and long-term prognoses compared with those with non-recovery. Numerous studies focus on biomarkers to distinguish them. To better understand the predictive performance of urinary biomarkers of renal recovery in patients with AKI, we evaluated C-C motif chemokine ligand 14 (CCL14) and two first-generation biomarkers (cell cycle arrest biomarkers and neutrophil gelatinase-associated lipocalin) in two ICU settings.</p><p><strong>Methods: </strong>We performed a prospective study to analyze urinary biomarkers for predicting renal recovery from AKI. Patients who developed AKI after ICU admission were enrolled and urinary biomarkers including tissue inhibitor of metalloproteinase-2 (TIMP-2), insulin-like growth factor-binding protein 7 (IGFBP7), CCL14, and neutrophil gelatinase-associated lipocalin (NGAL) were detected on the day of AKI diagnosis. The primary endpoint was non-recovery from AKI within 7 days. The individual discriminative ability of CCL14, [TIMP-2] × [IGFBP7] and NGAL to predict renal non-recovery were evaluated by the area under receiver operating characteristics curve (AUC).</p><p><strong>Results: </strong>Of 164 AKI patients, 64 (39.0%) failed to recover from AKI onset. CCL14 showed a fair prediction ability for renal non-recovery with an AUC of 0.71 (95% CI 0.63-0.77, p < 0.001). [TIMP-2] × [IGFBP7] showed the best prediction for renal non-recovery with an AUC of 0.78 (95% CI 0.71-0.84, p < 0.001). However, NGAL had no use in predicting non-recovery with an AUC of 0.53 (95% CI 0.45-0.60, p = 0.562). A two-parameter model (non-renal SOFA score and AKI stage) predicted renal non-recovery with an AUC of 0.77 (95% CI 0.77-0.83, p = 0.004). When [TIMP-2] × [IGFBP7] was combined with the clinical factors, the AUC was significantly improved to 0.82 (95% CI 0.74-0.87, p = 0.049).</p><p><strong>Conclusions: </strong>Urinary CCL14 and [TIMP-2] × [IGFBP7] were fair predictors of renal non-recovery from AKI. Combing urinary [TIMP-2] × [IGFBP7] with a clinical model consisting of non-renal SOFA score and AKI stage enhanced the predictive power for renal non-recovery. Urinary CCL14 showed no significant advantage in predicting renal non-recovery compared to [TIMP-2] × [IGFBP7].</p>\",\"PeriodicalId\":16123,\"journal\":{\"name\":\"Journal of Intensive Care\",\"volume\":\"11 1\",\"pages\":\"11\"},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2023-03-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10026399/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Intensive Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s40560-023-00659-2\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-023-00659-2","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Analysis of urinary C-C motif chemokine ligand 14 (CCL14) and first-generation urinary biomarkers for predicting renal recovery from acute kidney injury: a prospective exploratory study.
Background: Acute kidney injury (AKI) is a frequent syndrome in the intensive care unit (ICU). AKI patients with kidney function recovery have better short-term and long-term prognoses compared with those with non-recovery. Numerous studies focus on biomarkers to distinguish them. To better understand the predictive performance of urinary biomarkers of renal recovery in patients with AKI, we evaluated C-C motif chemokine ligand 14 (CCL14) and two first-generation biomarkers (cell cycle arrest biomarkers and neutrophil gelatinase-associated lipocalin) in two ICU settings.
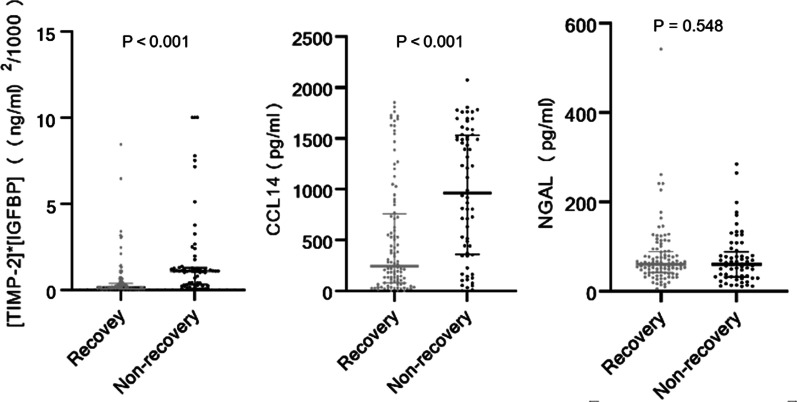
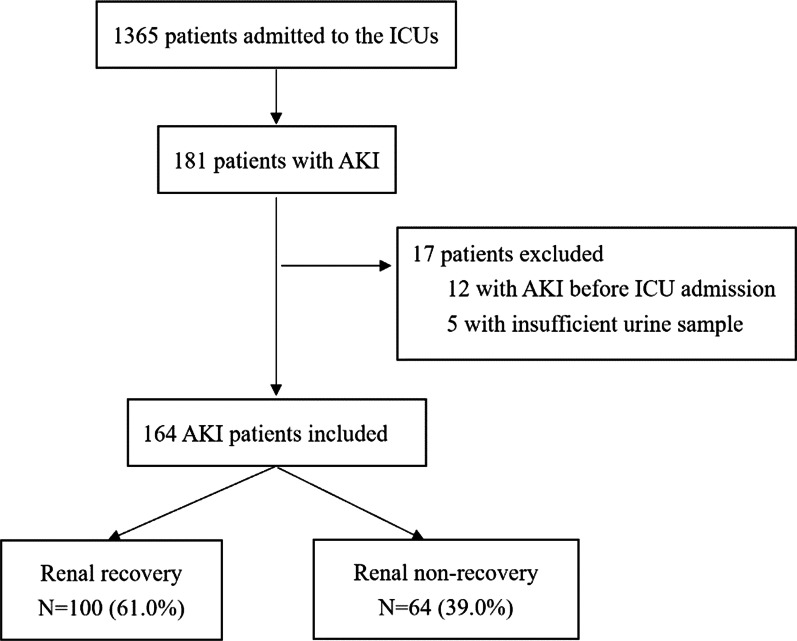
Methods: We performed a prospective study to analyze urinary biomarkers for predicting renal recovery from AKI. Patients who developed AKI after ICU admission were enrolled and urinary biomarkers including tissue inhibitor of metalloproteinase-2 (TIMP-2), insulin-like growth factor-binding protein 7 (IGFBP7), CCL14, and neutrophil gelatinase-associated lipocalin (NGAL) were detected on the day of AKI diagnosis. The primary endpoint was non-recovery from AKI within 7 days. The individual discriminative ability of CCL14, [TIMP-2] × [IGFBP7] and NGAL to predict renal non-recovery were evaluated by the area under receiver operating characteristics curve (AUC).
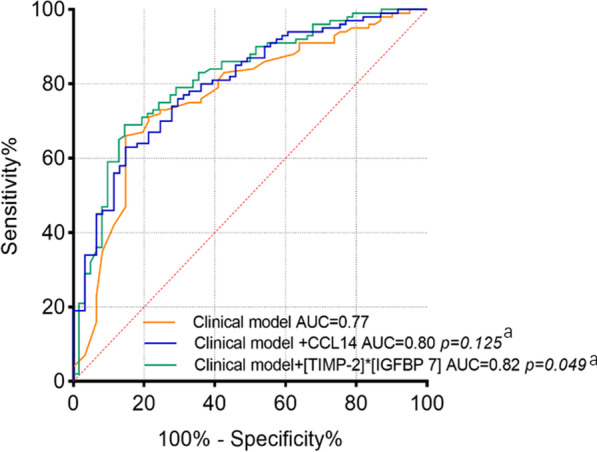
Results: Of 164 AKI patients, 64 (39.0%) failed to recover from AKI onset. CCL14 showed a fair prediction ability for renal non-recovery with an AUC of 0.71 (95% CI 0.63-0.77, p < 0.001). [TIMP-2] × [IGFBP7] showed the best prediction for renal non-recovery with an AUC of 0.78 (95% CI 0.71-0.84, p < 0.001). However, NGAL had no use in predicting non-recovery with an AUC of 0.53 (95% CI 0.45-0.60, p = 0.562). A two-parameter model (non-renal SOFA score and AKI stage) predicted renal non-recovery with an AUC of 0.77 (95% CI 0.77-0.83, p = 0.004). When [TIMP-2] × [IGFBP7] was combined with the clinical factors, the AUC was significantly improved to 0.82 (95% CI 0.74-0.87, p = 0.049).
Conclusions: Urinary CCL14 and [TIMP-2] × [IGFBP7] were fair predictors of renal non-recovery from AKI. Combing urinary [TIMP-2] × [IGFBP7] with a clinical model consisting of non-renal SOFA score and AKI stage enhanced the predictive power for renal non-recovery. Urinary CCL14 showed no significant advantage in predicting renal non-recovery compared to [TIMP-2] × [IGFBP7].
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


