Alison Garber, Pamela Garabedian, Lindsey Wu, Alyssa Lam, Maria Malik, Hannah Fraser, Kerrin Bersani, Nicholas Piniella, Daniel Motta-Calderon, Ronen Rozenblum, Kumiko Schnock, Jacqueline Griffin, Jeffrey L Schnipper, David W Bates, Anuj K Dalal
{"title":"开发、试点测试和完善 3 项电子病历集成干预措施的要求,以改善急症护理中的诊断安全:以用户为中心的方法。","authors":"Alison Garber, Pamela Garabedian, Lindsey Wu, Alyssa Lam, Maria Malik, Hannah Fraser, Kerrin Bersani, Nicholas Piniella, Daniel Motta-Calderon, Ronen Rozenblum, Kumiko Schnock, Jacqueline Griffin, Jeffrey L Schnipper, David W Bates, Anuj K Dalal","doi":"10.1093/jamiaopen/ooad031","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To describe a user-centered approach to develop, pilot test, and refine requirements for 3 electronic health record (EHR)-integrated interventions that target key diagnostic process failures in hospitalized patients.</p><p><strong>Materials and methods: </strong>Three interventions were prioritized for development: a Diagnostic Safety Column (<i>DSC</i>) within an EHR-integrated dashboard to identify at-risk patients; a Diagnostic Time-Out (<i>DTO</i>) for clinicians to reassess the working diagnosis; and a Patient Diagnosis Questionnaire (<i>PDQ</i>) to gather patient concerns about the diagnostic process. Initial requirements were refined from analysis of test cases with elevated risk predicted by <i>DSC</i> logic compared to risk perceived by a clinician working group; <i>DTO</i> testing sessions with clinicians; <i>PDQ</i> responses from patients; and focus groups with clinicians and patient advisors using storyboarding to model the integrated interventions. Mixed methods analysis of participant responses was used to identify final requirements and potential implementation barriers.</p><p><strong>Results: </strong>Final requirements from analysis of 10 test cases predicted by the <i>DSC</i>, 18 clinician <i>DTO</i> participants, and 39 <i>PDQ</i> responses included the following: <i>DSC</i> configurable parameters (variables, weights) to adjust baseline risk estimates in real-time based on new clinical data collected during hospitalization; more concise <i>DTO</i> wording and flexibility for clinicians to conduct the <i>DTO</i> with or without the patient present; and integration of <i>PDQ</i> responses into the <i>DSC</i> to ensure closed-looped communication with clinicians. Analysis of focus groups confirmed that tight integration of the interventions with the EHR would be necessary to prompt clinicians to reconsider the working diagnosis in cases with elevated diagnostic error (DE) risk or uncertainty. Potential implementation barriers included alert fatigue and distrust of the risk algorithm (<i>DSC</i>); time constraints, redundancies, and concerns about disclosing uncertainty to patients (<i>DTO</i>); and patient disagreement with the care team's diagnosis (<i>PDQ</i>).</p><p><strong>Discussion: </strong>A user-centered approach led to evolution of requirements for 3 interventions targeting key diagnostic process failures in hospitalized patients at risk for DE.</p><p><strong>Conclusions: </strong>We identify challenges and offer lessons from our user-centered design process.</p>","PeriodicalId":36278,"journal":{"name":"JAMIA Open","volume":"6 2","pages":"ooad031"},"PeriodicalIF":2.5000,"publicationDate":"2023-05-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a6/b8/ooad031.PMC10172040.pdf","citationCount":"0","resultStr":"{\"title\":\"Developing, pilot testing, and refining requirements for 3 EHR-integrated interventions to improve diagnostic safety in acute care: a user-centered approach.\",\"authors\":\"Alison Garber, Pamela Garabedian, Lindsey Wu, Alyssa Lam, Maria Malik, Hannah Fraser, Kerrin Bersani, Nicholas Piniella, Daniel Motta-Calderon, Ronen Rozenblum, Kumiko Schnock, Jacqueline Griffin, Jeffrey L Schnipper, David W Bates, Anuj K Dalal\",\"doi\":\"10.1093/jamiaopen/ooad031\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To describe a user-centered approach to develop, pilot test, and refine requirements for 3 electronic health record (EHR)-integrated interventions that target key diagnostic process failures in hospitalized patients.</p><p><strong>Materials and methods: </strong>Three interventions were prioritized for development: a Diagnostic Safety Column (<i>DSC</i>) within an EHR-integrated dashboard to identify at-risk patients; a Diagnostic Time-Out (<i>DTO</i>) for clinicians to reassess the working diagnosis; and a Patient Diagnosis Questionnaire (<i>PDQ</i>) to gather patient concerns about the diagnostic process. Initial requirements were refined from analysis of test cases with elevated risk predicted by <i>DSC</i> logic compared to risk perceived by a clinician working group; <i>DTO</i> testing sessions with clinicians; <i>PDQ</i> responses from patients; and focus groups with clinicians and patient advisors using storyboarding to model the integrated interventions. Mixed methods analysis of participant responses was used to identify final requirements and potential implementation barriers.</p><p><strong>Results: </strong>Final requirements from analysis of 10 test cases predicted by the <i>DSC</i>, 18 clinician <i>DTO</i> participants, and 39 <i>PDQ</i> responses included the following: <i>DSC</i> configurable parameters (variables, weights) to adjust baseline risk estimates in real-time based on new clinical data collected during hospitalization; more concise <i>DTO</i> wording and flexibility for clinicians to conduct the <i>DTO</i> with or without the patient present; and integration of <i>PDQ</i> responses into the <i>DSC</i> to ensure closed-looped communication with clinicians. Analysis of focus groups confirmed that tight integration of the interventions with the EHR would be necessary to prompt clinicians to reconsider the working diagnosis in cases with elevated diagnostic error (DE) risk or uncertainty. Potential implementation barriers included alert fatigue and distrust of the risk algorithm (<i>DSC</i>); time constraints, redundancies, and concerns about disclosing uncertainty to patients (<i>DTO</i>); and patient disagreement with the care team's diagnosis (<i>PDQ</i>).</p><p><strong>Discussion: </strong>A user-centered approach led to evolution of requirements for 3 interventions targeting key diagnostic process failures in hospitalized patients at risk for DE.</p><p><strong>Conclusions: </strong>We identify challenges and offer lessons from our user-centered design process.</p>\",\"PeriodicalId\":36278,\"journal\":{\"name\":\"JAMIA Open\",\"volume\":\"6 2\",\"pages\":\"ooad031\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2023-05-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a6/b8/ooad031.PMC10172040.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JAMIA Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/jamiaopen/ooad031\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMIA Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jamiaopen/ooad031","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Developing, pilot testing, and refining requirements for 3 EHR-integrated interventions to improve diagnostic safety in acute care: a user-centered approach.
Objective: To describe a user-centered approach to develop, pilot test, and refine requirements for 3 electronic health record (EHR)-integrated interventions that target key diagnostic process failures in hospitalized patients.
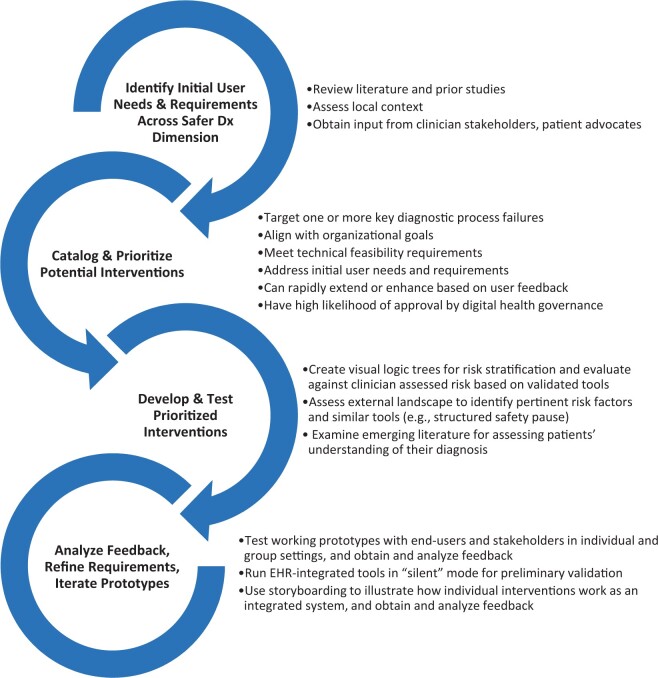
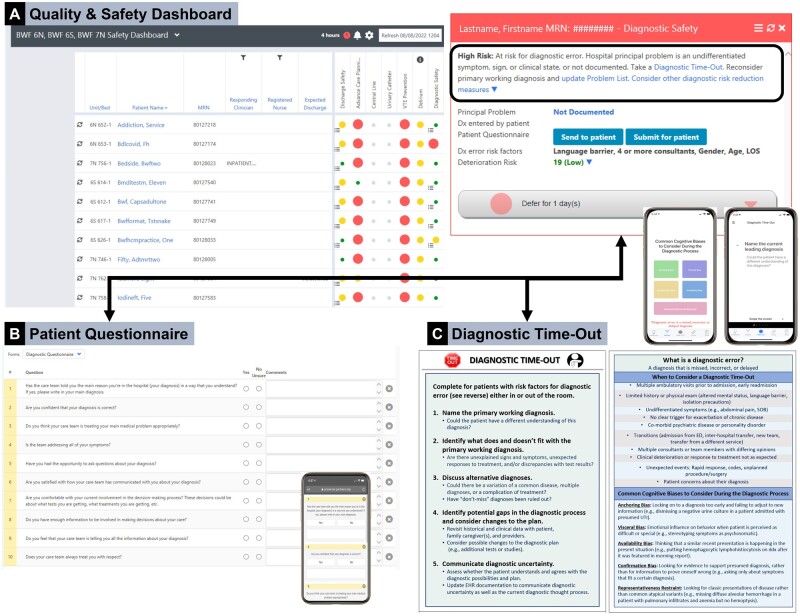
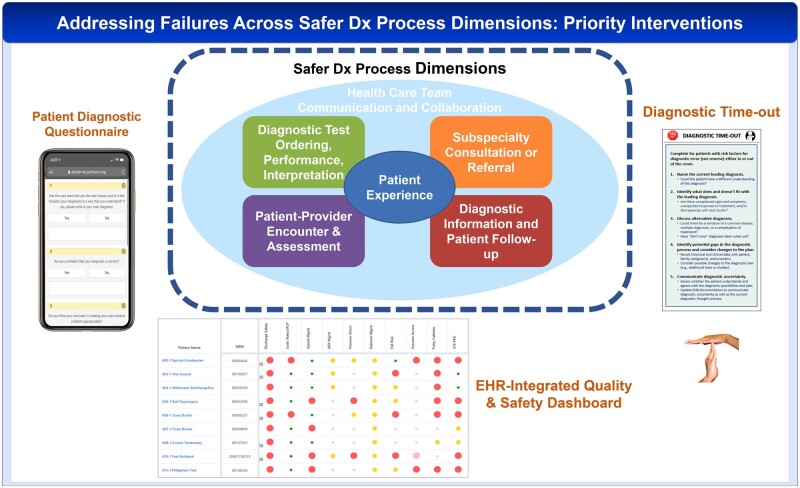
Materials and methods: Three interventions were prioritized for development: a Diagnostic Safety Column (DSC) within an EHR-integrated dashboard to identify at-risk patients; a Diagnostic Time-Out (DTO) for clinicians to reassess the working diagnosis; and a Patient Diagnosis Questionnaire (PDQ) to gather patient concerns about the diagnostic process. Initial requirements were refined from analysis of test cases with elevated risk predicted by DSC logic compared to risk perceived by a clinician working group; DTO testing sessions with clinicians; PDQ responses from patients; and focus groups with clinicians and patient advisors using storyboarding to model the integrated interventions. Mixed methods analysis of participant responses was used to identify final requirements and potential implementation barriers.
Results: Final requirements from analysis of 10 test cases predicted by the DSC, 18 clinician DTO participants, and 39 PDQ responses included the following: DSC configurable parameters (variables, weights) to adjust baseline risk estimates in real-time based on new clinical data collected during hospitalization; more concise DTO wording and flexibility for clinicians to conduct the DTO with or without the patient present; and integration of PDQ responses into the DSC to ensure closed-looped communication with clinicians. Analysis of focus groups confirmed that tight integration of the interventions with the EHR would be necessary to prompt clinicians to reconsider the working diagnosis in cases with elevated diagnostic error (DE) risk or uncertainty. Potential implementation barriers included alert fatigue and distrust of the risk algorithm (DSC); time constraints, redundancies, and concerns about disclosing uncertainty to patients (DTO); and patient disagreement with the care team's diagnosis (PDQ).
Discussion: A user-centered approach led to evolution of requirements for 3 interventions targeting key diagnostic process failures in hospitalized patients at risk for DE.
Conclusions: We identify challenges and offer lessons from our user-centered design process.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


