Toshiaki Iba, Julie Helms, Jean Marie Connors, Jerrold H Levy
{"title":"脓毒症相关弥散性血管内凝血的病理生理学、诊断和治疗。","authors":"Toshiaki Iba, Julie Helms, Jean Marie Connors, Jerrold H Levy","doi":"10.1186/s40560-023-00672-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The International Society on Thrombosis and Haemostasis (ISTH) released overt disseminated intravascular coagulation (DIC) diagnostic criteria in 2001. Since then, DIC has been understood as the end-stage consumptive coagulopathy and not the therapeutic target. However, DIC is not merely a decompensated coagulation disorder, but also includes early stages with systemic activation in coagulation. Thus, the ISTH has recently released sepsis-induced coagulopathy (SIC) criteria that can diagnose compensated-phase of coagulopathy with readily available biomarkers.</p><p><strong>Main body: </strong>DIC is a laboratory-based diagnosis due to various critical conditions, although sepsis is the most common underlying disease. The pathophysiology of sepsis-associated DIC is multifactorial, and in addition to coagulation activation with suppressed fibrinolysis, multiple inflammatory responses are initiated by activated leukocytes, platelets, and vascular endothelial cells as part of thromboinflammation. Although overt DIC diagnostic criteria were established by ISTH to diagnose the advanced stage of DIC, additional criteria that can detect an earlier stage of DIC were needed for potential therapeutic considerations. Accordingly, the ISTH introduced SIC criteria in 2019 that are easy to use and require only platelet count, prothrombin time-international normalized ratio, and Sequential Organ Failure Assessment Score. SIC score can be used to evaluate disease severity and determine the timing of potential therapeutic interventions. One of the major disadvantages in treating sepsis-associated DIC is the lack of availability of specific therapeutic approaches beyond treating the underlying infection. Clinical trials to date have failed because included patients who were not coagulopathic. Nevertheless, in addition to infection control, anticoagulant therapy will be the choice for sepsis-associated DIC. Therefore, the efficacy of heparin, antithrombin, and recombinant thrombomodulin has to be proven in future clinical studies.</p><p><strong>Conclusion: </strong>It is necessary to develop a novel therapeutic strategy against sepsis-associated DIC and improve the outcomes. Consequently, we recommend screening and monitoring DIC using SIC scoring system.</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":null,"pages":null},"PeriodicalIF":3.8000,"publicationDate":"2023-05-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10202753/pdf/","citationCount":"5","resultStr":"{\"title\":\"The pathophysiology, diagnosis, and management of sepsis-associated disseminated intravascular coagulation.\",\"authors\":\"Toshiaki Iba, Julie Helms, Jean Marie Connors, Jerrold H Levy\",\"doi\":\"10.1186/s40560-023-00672-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The International Society on Thrombosis and Haemostasis (ISTH) released overt disseminated intravascular coagulation (DIC) diagnostic criteria in 2001. Since then, DIC has been understood as the end-stage consumptive coagulopathy and not the therapeutic target. However, DIC is not merely a decompensated coagulation disorder, but also includes early stages with systemic activation in coagulation. Thus, the ISTH has recently released sepsis-induced coagulopathy (SIC) criteria that can diagnose compensated-phase of coagulopathy with readily available biomarkers.</p><p><strong>Main body: </strong>DIC is a laboratory-based diagnosis due to various critical conditions, although sepsis is the most common underlying disease. The pathophysiology of sepsis-associated DIC is multifactorial, and in addition to coagulation activation with suppressed fibrinolysis, multiple inflammatory responses are initiated by activated leukocytes, platelets, and vascular endothelial cells as part of thromboinflammation. Although overt DIC diagnostic criteria were established by ISTH to diagnose the advanced stage of DIC, additional criteria that can detect an earlier stage of DIC were needed for potential therapeutic considerations. Accordingly, the ISTH introduced SIC criteria in 2019 that are easy to use and require only platelet count, prothrombin time-international normalized ratio, and Sequential Organ Failure Assessment Score. SIC score can be used to evaluate disease severity and determine the timing of potential therapeutic interventions. One of the major disadvantages in treating sepsis-associated DIC is the lack of availability of specific therapeutic approaches beyond treating the underlying infection. Clinical trials to date have failed because included patients who were not coagulopathic. Nevertheless, in addition to infection control, anticoagulant therapy will be the choice for sepsis-associated DIC. Therefore, the efficacy of heparin, antithrombin, and recombinant thrombomodulin has to be proven in future clinical studies.</p><p><strong>Conclusion: </strong>It is necessary to develop a novel therapeutic strategy against sepsis-associated DIC and improve the outcomes. Consequently, we recommend screening and monitoring DIC using SIC scoring system.</p>\",\"PeriodicalId\":16123,\"journal\":{\"name\":\"Journal of Intensive Care\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2023-05-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10202753/pdf/\",\"citationCount\":\"5\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Intensive Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s40560-023-00672-5\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-023-00672-5","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
The pathophysiology, diagnosis, and management of sepsis-associated disseminated intravascular coagulation.
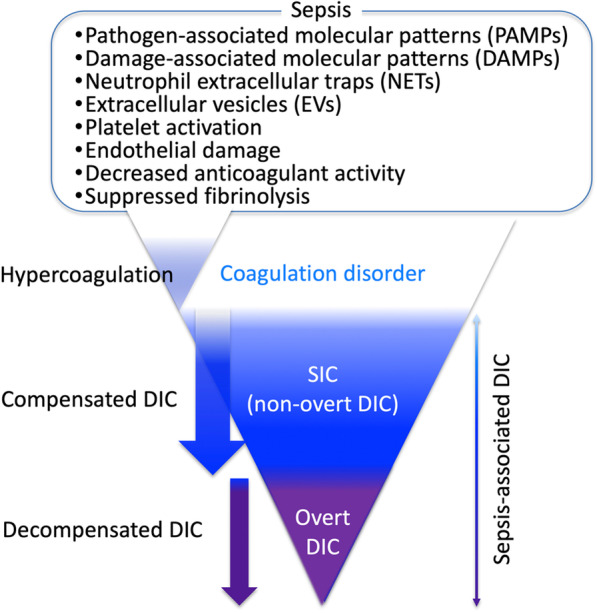
Background: The International Society on Thrombosis and Haemostasis (ISTH) released overt disseminated intravascular coagulation (DIC) diagnostic criteria in 2001. Since then, DIC has been understood as the end-stage consumptive coagulopathy and not the therapeutic target. However, DIC is not merely a decompensated coagulation disorder, but also includes early stages with systemic activation in coagulation. Thus, the ISTH has recently released sepsis-induced coagulopathy (SIC) criteria that can diagnose compensated-phase of coagulopathy with readily available biomarkers.
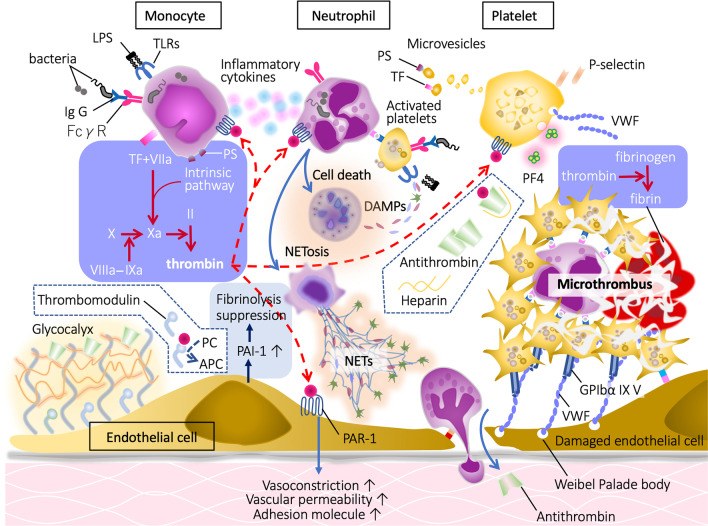
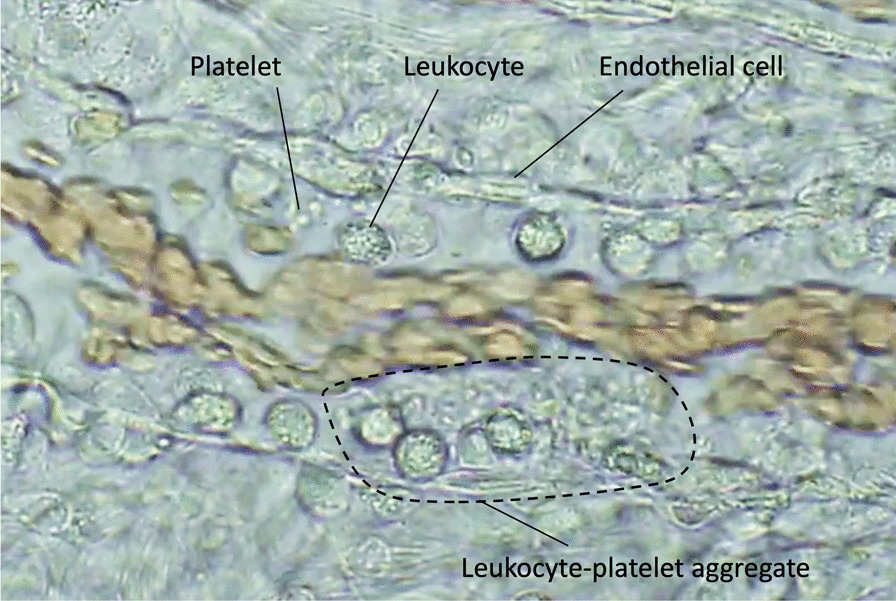
Main body: DIC is a laboratory-based diagnosis due to various critical conditions, although sepsis is the most common underlying disease. The pathophysiology of sepsis-associated DIC is multifactorial, and in addition to coagulation activation with suppressed fibrinolysis, multiple inflammatory responses are initiated by activated leukocytes, platelets, and vascular endothelial cells as part of thromboinflammation. Although overt DIC diagnostic criteria were established by ISTH to diagnose the advanced stage of DIC, additional criteria that can detect an earlier stage of DIC were needed for potential therapeutic considerations. Accordingly, the ISTH introduced SIC criteria in 2019 that are easy to use and require only platelet count, prothrombin time-international normalized ratio, and Sequential Organ Failure Assessment Score. SIC score can be used to evaluate disease severity and determine the timing of potential therapeutic interventions. One of the major disadvantages in treating sepsis-associated DIC is the lack of availability of specific therapeutic approaches beyond treating the underlying infection. Clinical trials to date have failed because included patients who were not coagulopathic. Nevertheless, in addition to infection control, anticoagulant therapy will be the choice for sepsis-associated DIC. Therefore, the efficacy of heparin, antithrombin, and recombinant thrombomodulin has to be proven in future clinical studies.
Conclusion: It is necessary to develop a novel therapeutic strategy against sepsis-associated DIC and improve the outcomes. Consequently, we recommend screening and monitoring DIC using SIC scoring system.
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


