John Heintzman, Dang Dinh, Jennifer A Lucas, Elena Byhoff, Danielle M Crookes, Ayana April-Sanders, Jorge Kaufmann, Dave Boston, Audree Hsu, Sophia Giebultowicz, Miguel Marino
{"title":"响应严格的健康公平研究号召:利用电子健康记录对拉丁裔进行数据分类的横断面研究。","authors":"John Heintzman, Dang Dinh, Jennifer A Lucas, Elena Byhoff, Danielle M Crookes, Ayana April-Sanders, Jorge Kaufmann, Dave Boston, Audree Hsu, Sophia Giebultowicz, Miguel Marino","doi":"10.1136/fmch-2022-001972","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Country of birth/nativity information may be crucial to understanding health equity in Latino populations and is routinely called for in health services literature assessing cardiovascular disease and risk, but is not thought to co-occur with longitudinal, objective health information such as that found in electronic health records (EHRs).</p><p><strong>Methods: </strong>We used a multistate network of community health centres to describe the extent to which country of birth is recorded in EHRs in Latinos, and to describe demographic features and cardiovascular risk profiles by country of birth. We compared geographical/demographic/clinical characteristics, from 2012 to 2020 (9 years of data), of 914 495 Latinos recorded as US-born, non-US-born and without a country of birth recorded. We also described the state in which these data were collected.</p><p><strong>Results: </strong>Country of birth was collected for 127 138 Latinos in 782 clinics in 22 states. Compared with those with a country of birth recorded, Latinos without this record were more often uninsured and less often preferred Spanish. While covariate adjusted prevalence of heart disease and risk factors were similar between the three groups, when results were disaggregated to five specific Latin countries (Mexico, Guatemala, Dominican Republic, Cuba, El Salvador), significant variation was observed, especially in diabetes, hypertension and hyperlipidaemia.</p><p><strong>Conclusions: </strong>In a multistate network, thousands of non-US-born, US-born and patients without a country of birth recorded had differing demographic characteristics, but clinical variation was not observed until data was disaggregated into specific country of origin. State policies that enhance the safety of immigrant populations may enhance the collection of health equity related data. Rigorous and effective health equity research using Latino country of birth information paired with longitudinal healthcare information found in EHRs might have significant potential for aiding clinical and public health practice, but it depends on increased, widespread and accurate availability of this information, co-occurring with other robust demographic and clinical data nativity.</p>","PeriodicalId":44590,"journal":{"name":"Family Medicine and Community Health","volume":"11 2","pages":""},"PeriodicalIF":4.3000,"publicationDate":"2023-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/59/08/fmch-2022-001972.PMC10186452.pdf","citationCount":"0","resultStr":"{\"title\":\"Answering calls for rigorous health equity research: a cross-sectional study leveraging electronic health records for data disaggregation in Latinos.\",\"authors\":\"John Heintzman, Dang Dinh, Jennifer A Lucas, Elena Byhoff, Danielle M Crookes, Ayana April-Sanders, Jorge Kaufmann, Dave Boston, Audree Hsu, Sophia Giebultowicz, Miguel Marino\",\"doi\":\"10.1136/fmch-2022-001972\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Country of birth/nativity information may be crucial to understanding health equity in Latino populations and is routinely called for in health services literature assessing cardiovascular disease and risk, but is not thought to co-occur with longitudinal, objective health information such as that found in electronic health records (EHRs).</p><p><strong>Methods: </strong>We used a multistate network of community health centres to describe the extent to which country of birth is recorded in EHRs in Latinos, and to describe demographic features and cardiovascular risk profiles by country of birth. We compared geographical/demographic/clinical characteristics, from 2012 to 2020 (9 years of data), of 914 495 Latinos recorded as US-born, non-US-born and without a country of birth recorded. We also described the state in which these data were collected.</p><p><strong>Results: </strong>Country of birth was collected for 127 138 Latinos in 782 clinics in 22 states. Compared with those with a country of birth recorded, Latinos without this record were more often uninsured and less often preferred Spanish. While covariate adjusted prevalence of heart disease and risk factors were similar between the three groups, when results were disaggregated to five specific Latin countries (Mexico, Guatemala, Dominican Republic, Cuba, El Salvador), significant variation was observed, especially in diabetes, hypertension and hyperlipidaemia.</p><p><strong>Conclusions: </strong>In a multistate network, thousands of non-US-born, US-born and patients without a country of birth recorded had differing demographic characteristics, but clinical variation was not observed until data was disaggregated into specific country of origin. State policies that enhance the safety of immigrant populations may enhance the collection of health equity related data. Rigorous and effective health equity research using Latino country of birth information paired with longitudinal healthcare information found in EHRs might have significant potential for aiding clinical and public health practice, but it depends on increased, widespread and accurate availability of this information, co-occurring with other robust demographic and clinical data nativity.</p>\",\"PeriodicalId\":44590,\"journal\":{\"name\":\"Family Medicine and Community Health\",\"volume\":\"11 2\",\"pages\":\"\"},\"PeriodicalIF\":4.3000,\"publicationDate\":\"2023-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/59/08/fmch-2022-001972.PMC10186452.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Family Medicine and Community Health\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/fmch-2022-001972\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PRIMARY HEALTH CARE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Family Medicine and Community Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/fmch-2022-001972","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PRIMARY HEALTH CARE","Score":null,"Total":0}
Answering calls for rigorous health equity research: a cross-sectional study leveraging electronic health records for data disaggregation in Latinos.
Introduction: Country of birth/nativity information may be crucial to understanding health equity in Latino populations and is routinely called for in health services literature assessing cardiovascular disease and risk, but is not thought to co-occur with longitudinal, objective health information such as that found in electronic health records (EHRs).
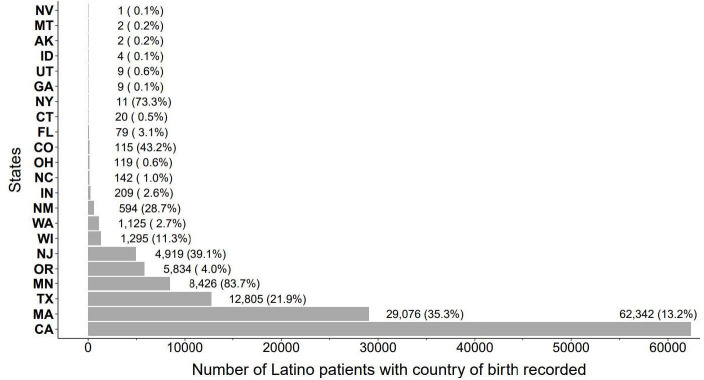
Methods: We used a multistate network of community health centres to describe the extent to which country of birth is recorded in EHRs in Latinos, and to describe demographic features and cardiovascular risk profiles by country of birth. We compared geographical/demographic/clinical characteristics, from 2012 to 2020 (9 years of data), of 914 495 Latinos recorded as US-born, non-US-born and without a country of birth recorded. We also described the state in which these data were collected.
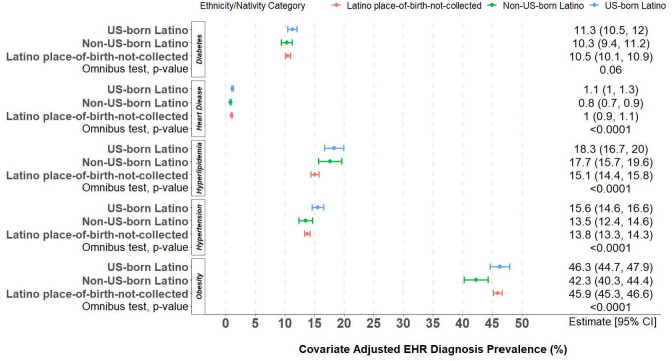
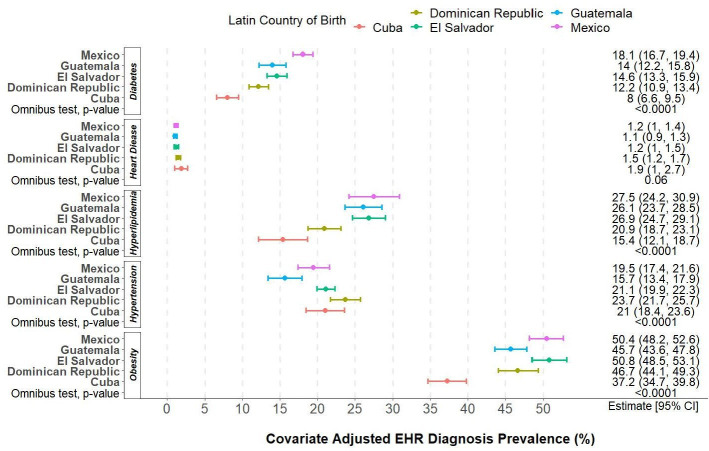
Results: Country of birth was collected for 127 138 Latinos in 782 clinics in 22 states. Compared with those with a country of birth recorded, Latinos without this record were more often uninsured and less often preferred Spanish. While covariate adjusted prevalence of heart disease and risk factors were similar between the three groups, when results were disaggregated to five specific Latin countries (Mexico, Guatemala, Dominican Republic, Cuba, El Salvador), significant variation was observed, especially in diabetes, hypertension and hyperlipidaemia.
Conclusions: In a multistate network, thousands of non-US-born, US-born and patients without a country of birth recorded had differing demographic characteristics, but clinical variation was not observed until data was disaggregated into specific country of origin. State policies that enhance the safety of immigrant populations may enhance the collection of health equity related data. Rigorous and effective health equity research using Latino country of birth information paired with longitudinal healthcare information found in EHRs might have significant potential for aiding clinical and public health practice, but it depends on increased, widespread and accurate availability of this information, co-occurring with other robust demographic and clinical data nativity.
期刊介绍:
Family Medicine and Community Health (FMCH) is a peer-reviewed, open-access journal focusing on the topics of family medicine, general practice and community health. FMCH strives to be a leading international journal that promotes ‘Health Care for All’ through disseminating novel knowledge and best practices in primary care, family medicine, and community health. FMCH publishes original research, review, methodology, commentary, reflection, and case-study from the lens of population health. FMCH’s Asian Focus section features reports of family medicine development in the Asia-pacific region. FMCH aims to be an exemplary forum for the timely communication of medical knowledge and skills with the goal of promoting improved health care through the practice of family and community-based medicine globally. FMCH aims to serve a diverse audience including researchers, educators, policymakers and leaders of family medicine and community health. We also aim to provide content relevant for researchers working on population health, epidemiology, public policy, disease control and management, preventative medicine and disease burden. FMCH does not impose any article processing charges (APC) or submission charges.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


