Ana Tejedor, Carme Deiros, Lana Bijelic, Marta García
{"title":"腹腔镜根治性前列腺切除术后伤口浸润或腹横面阻滞:一项随机临床试验。","authors":"Ana Tejedor, Carme Deiros, Lana Bijelic, Marta García","doi":"10.17085/apm.23005","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Regional anesthesia techniques are commonly used for postoperative pain management during laparoscopic surgery. Our aim was to compare the analgesic efficacy of pre-incisional subcutaneous wound infiltration (WI) with that of the transversus abdominis plane (TAP) block as part of a multimodal analgesic approach in laparoscopic radical prostatectomy.</p><p><strong>Methods: </strong>In this prospective, double-blinded, randomized controlled clinical trial, 60 patients were assigned to either TAP or WI group. The main outcome was acute postoperative pain control assessed using the mean numeric rating scale (NRS) at the 24 hours postoperatively. The secondary outcomes were opioid requirements, procedure-related complications, overall complications, and length of stay.</p><p><strong>Results: </strong>In this study, 60 patients were randomized: 30 to TAP group and 28 to WI (two were excluded due to conversion to open surgery). We found no significant difference in the median (1Q, 3Q) NRS scores during the 24 h postoperatively neither at rest (TAP, 0 (0, 1) vs. WI, 0 (0, 1), P = 0.812), nor during movement (TAP, 1 (0, 2) vs. WI, 1 (0, 2), P = 0.708). There were no statistical differences in the postoperative intravenous morphine requirements in the TAP vs. WI groups during the same period (1.7 ± 3.1 vs. 1.8 ± 4.1 mg; P = 0.910). Only one patient in the TAP group presented with postoperative nausea and vomiting.</p><p><strong>Conclusions: </strong>Both pre-incisional subcutaneous WI and TAP blockade were associated with very low pain scores as part of a non-opioid multimodal analgesic regimen in laparoscopic radical prostatectomy. This study did not demonstrate the benefits of WI over TAP.</p>","PeriodicalId":7801,"journal":{"name":"Anesthesia and pain medicine","volume":"18 2","pages":"190-197"},"PeriodicalIF":0.0000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/49/24/apm-23005.PMC10183622.pdf","citationCount":"0","resultStr":"{\"title\":\"Wound infiltration or transversus abdominis plane block after laparoscopic radical prostatectomy: a randomized clinical trial.\",\"authors\":\"Ana Tejedor, Carme Deiros, Lana Bijelic, Marta García\",\"doi\":\"10.17085/apm.23005\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Regional anesthesia techniques are commonly used for postoperative pain management during laparoscopic surgery. Our aim was to compare the analgesic efficacy of pre-incisional subcutaneous wound infiltration (WI) with that of the transversus abdominis plane (TAP) block as part of a multimodal analgesic approach in laparoscopic radical prostatectomy.</p><p><strong>Methods: </strong>In this prospective, double-blinded, randomized controlled clinical trial, 60 patients were assigned to either TAP or WI group. The main outcome was acute postoperative pain control assessed using the mean numeric rating scale (NRS) at the 24 hours postoperatively. The secondary outcomes were opioid requirements, procedure-related complications, overall complications, and length of stay.</p><p><strong>Results: </strong>In this study, 60 patients were randomized: 30 to TAP group and 28 to WI (two were excluded due to conversion to open surgery). We found no significant difference in the median (1Q, 3Q) NRS scores during the 24 h postoperatively neither at rest (TAP, 0 (0, 1) vs. WI, 0 (0, 1), P = 0.812), nor during movement (TAP, 1 (0, 2) vs. WI, 1 (0, 2), P = 0.708). There were no statistical differences in the postoperative intravenous morphine requirements in the TAP vs. WI groups during the same period (1.7 ± 3.1 vs. 1.8 ± 4.1 mg; P = 0.910). Only one patient in the TAP group presented with postoperative nausea and vomiting.</p><p><strong>Conclusions: </strong>Both pre-incisional subcutaneous WI and TAP blockade were associated with very low pain scores as part of a non-opioid multimodal analgesic regimen in laparoscopic radical prostatectomy. This study did not demonstrate the benefits of WI over TAP.</p>\",\"PeriodicalId\":7801,\"journal\":{\"name\":\"Anesthesia and pain medicine\",\"volume\":\"18 2\",\"pages\":\"190-197\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/49/24/apm-23005.PMC10183622.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Anesthesia and pain medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.17085/apm.23005\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesia and pain medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17085/apm.23005","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:区域麻醉技术通常用于腹腔镜手术术后疼痛管理。我们的目的是比较切开前皮下伤口浸润(WI)和腹横面阻滞(TAP)作为腹腔镜根治性前列腺切除术多模式镇痛方法的一部分的镇痛效果。方法:在这项前瞻性、双盲、随机对照临床试验中,60例患者被分为TAP组和WI组。主要结果是术后24小时用平均数值评定量表(NRS)评估急性术后疼痛控制。次要结果是阿片类药物需求、手术相关并发症、总并发症和住院时间。结果:本研究随机选取60例患者:TAP组30例,WI组28例(2例因转为开放手术而被排除)。我们发现,在术后24小时内,无论是在休息时(TAP, 0 (0,1) vs. WI, 0 (0,1), P = 0.812),还是在运动时(TAP, 1 (0,2) vs. WI, 1 (0,2), P = 0.708),中位(1Q, 3Q) NRS评分均无显著差异。同期TAP组与WI组术后静脉吗啡需用量比较,差异无统计学意义(1.7±3.1 vs 1.8±4.1 mg;P = 0.910)。TAP组中仅有1例患者出现术后恶心和呕吐。结论:在腹腔镜根治性前列腺切除术中,作为非阿片类药物多模式镇痛方案的一部分,切开前皮下WI和TAP阻断与非常低的疼痛评分相关。这项研究并没有证明WI优于TAP。
Wound infiltration or transversus abdominis plane block after laparoscopic radical prostatectomy: a randomized clinical trial.
Background: Regional anesthesia techniques are commonly used for postoperative pain management during laparoscopic surgery. Our aim was to compare the analgesic efficacy of pre-incisional subcutaneous wound infiltration (WI) with that of the transversus abdominis plane (TAP) block as part of a multimodal analgesic approach in laparoscopic radical prostatectomy.
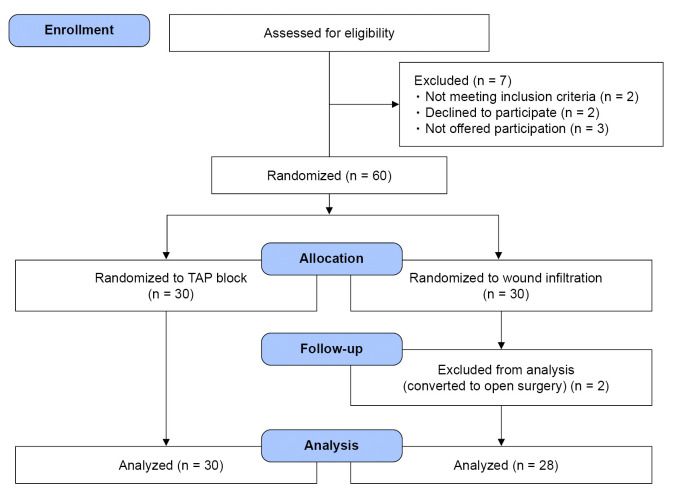
Methods: In this prospective, double-blinded, randomized controlled clinical trial, 60 patients were assigned to either TAP or WI group. The main outcome was acute postoperative pain control assessed using the mean numeric rating scale (NRS) at the 24 hours postoperatively. The secondary outcomes were opioid requirements, procedure-related complications, overall complications, and length of stay.
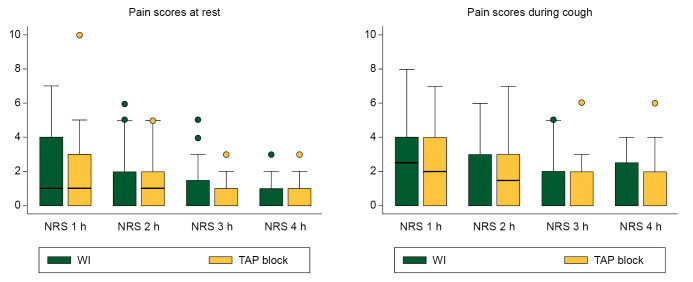
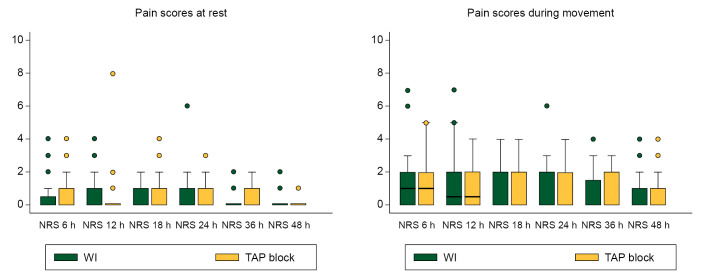
Results: In this study, 60 patients were randomized: 30 to TAP group and 28 to WI (two were excluded due to conversion to open surgery). We found no significant difference in the median (1Q, 3Q) NRS scores during the 24 h postoperatively neither at rest (TAP, 0 (0, 1) vs. WI, 0 (0, 1), P = 0.812), nor during movement (TAP, 1 (0, 2) vs. WI, 1 (0, 2), P = 0.708). There were no statistical differences in the postoperative intravenous morphine requirements in the TAP vs. WI groups during the same period (1.7 ± 3.1 vs. 1.8 ± 4.1 mg; P = 0.910). Only one patient in the TAP group presented with postoperative nausea and vomiting.
Conclusions: Both pre-incisional subcutaneous WI and TAP blockade were associated with very low pain scores as part of a non-opioid multimodal analgesic regimen in laparoscopic radical prostatectomy. This study did not demonstrate the benefits of WI over TAP.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


