{"title":"推导和验证一种新的风险评分来预测急性上消化道出血止血干预的需要(伦敦止血评分)。","authors":"Isobel Marks, Imran Karim Janmohamed, Sadek Malas, Athina Mavrou, Thomas Banister, Nisha Patel, Lakshmana Ayaru","doi":"10.1136/bmjgast-2022-001008","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute upper gastrointestinal bleeding (AUGIB) is a common medical emergency, which takes up considerable healthcare resources. However, only approximately 20%-30% of bleeds require urgent haemostatic intervention. Current standard of care is for all patients admitted to hospital to undergo endoscopy within 24 hours for risk stratification, but this is difficult to achieve in practice, invasive and costly.</p><p><strong>Aim: </strong>To develop a novel non-endoscopic risk stratification tool for AUGIB to predict the need for haemostatic intervention by endoscopic, radiological or surgical treatments. We compared this with the Glasgow-Blatchford Score (GBS).</p><p><strong>Design: </strong>Model development was carried out using a derivation (n=466) and prospectively collected validation cohort (n=404) of patients who were admitted with AUGIB to three large hospitals in London, UK (2015-2020). Univariable and multivariable logistic regression analysis was used to identify variables that were associated with increased or decreased chances of requiring haemostatic intervention. This model was converted into a risk scoring system, the London Haemostat Score (LHS).</p><p><strong>Results: </strong>The LHS was more accurate at predicting need for haemostatic intervention than the GBS, in the derivation cohort (area under the receiver operating curve (AUROC) 0.82; 95% CI 0.78 to 0.86 vs 0.72; 95% CI 0.67 to 0.77; p<0.001) and validation cohort (AUROC 0.80; 95% CI 0.75 to 0.85 vs 0.72; 95% CI 0.67 to 0.78; p<0.001). At cut-off scores at which LHS and GBS identified patients who required haemostatic intervention with 98% sensitivity, the specificity of the LHS was 41% vs 18% with the GBS (p<0.001). This could translate to 32% of inpatient endoscopies for AUGIB being avoided at a cost of only a 0.5% false negative rate.</p><p><strong>Conclusions: </strong>The LHS is accurate at predicting the need for haemostatic intervention in AUGIB and could be used to identify a proportion of low-risk patients who can undergo delayed or outpatient endoscopy. Validation in other geographical settings is required before routine clinical use.</p>","PeriodicalId":9235,"journal":{"name":"BMJ Open Gastroenterology","volume":null,"pages":null},"PeriodicalIF":3.3000,"publicationDate":"2023-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/dc/6b/bmjgast-2022-001008.PMC10069503.pdf","citationCount":"1","resultStr":"{\"title\":\"Derivation and validation of a novel risk score to predict need for haemostatic intervention in acute upper gastrointestinal bleeding (London Haemostat Score).\",\"authors\":\"Isobel Marks, Imran Karim Janmohamed, Sadek Malas, Athina Mavrou, Thomas Banister, Nisha Patel, Lakshmana Ayaru\",\"doi\":\"10.1136/bmjgast-2022-001008\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Acute upper gastrointestinal bleeding (AUGIB) is a common medical emergency, which takes up considerable healthcare resources. However, only approximately 20%-30% of bleeds require urgent haemostatic intervention. Current standard of care is for all patients admitted to hospital to undergo endoscopy within 24 hours for risk stratification, but this is difficult to achieve in practice, invasive and costly.</p><p><strong>Aim: </strong>To develop a novel non-endoscopic risk stratification tool for AUGIB to predict the need for haemostatic intervention by endoscopic, radiological or surgical treatments. We compared this with the Glasgow-Blatchford Score (GBS).</p><p><strong>Design: </strong>Model development was carried out using a derivation (n=466) and prospectively collected validation cohort (n=404) of patients who were admitted with AUGIB to three large hospitals in London, UK (2015-2020). Univariable and multivariable logistic regression analysis was used to identify variables that were associated with increased or decreased chances of requiring haemostatic intervention. This model was converted into a risk scoring system, the London Haemostat Score (LHS).</p><p><strong>Results: </strong>The LHS was more accurate at predicting need for haemostatic intervention than the GBS, in the derivation cohort (area under the receiver operating curve (AUROC) 0.82; 95% CI 0.78 to 0.86 vs 0.72; 95% CI 0.67 to 0.77; p<0.001) and validation cohort (AUROC 0.80; 95% CI 0.75 to 0.85 vs 0.72; 95% CI 0.67 to 0.78; p<0.001). At cut-off scores at which LHS and GBS identified patients who required haemostatic intervention with 98% sensitivity, the specificity of the LHS was 41% vs 18% with the GBS (p<0.001). This could translate to 32% of inpatient endoscopies for AUGIB being avoided at a cost of only a 0.5% false negative rate.</p><p><strong>Conclusions: </strong>The LHS is accurate at predicting the need for haemostatic intervention in AUGIB and could be used to identify a proportion of low-risk patients who can undergo delayed or outpatient endoscopy. Validation in other geographical settings is required before routine clinical use.</p>\",\"PeriodicalId\":9235,\"journal\":{\"name\":\"BMJ Open Gastroenterology\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2023-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/dc/6b/bmjgast-2022-001008.PMC10069503.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Open Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjgast-2022-001008\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjgast-2022-001008","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 1
摘要
背景:急性上消化道出血(AUGIB)是一种常见的急症,占用了大量的医疗资源。然而,只有大约20%-30%的出血需要紧急止血干预。目前的护理标准是所有入院患者在24小时内接受内镜检查以进行风险分层,但这在实践中难以实现,具有侵入性且费用昂贵。目的:为AUGIB开发一种新的非内镜风险分层工具,以预测通过内镜、放射或手术治疗进行止血干预的必要性。我们将其与格拉斯哥-布拉奇福德评分(GBS)进行了比较。设计:模型开发使用推导(n=466)和前瞻性收集的验证队列(n=404)进行,这些患者是2015-2020年在英国伦敦三家大医院接受AUGIB的患者。单变量和多变量logistic回归分析用于确定与需要止血干预的机会增加或减少相关的变量。该模型被转换成一个风险评分系统,即伦敦血肿评分(LHS)。结果:在衍生队列中,LHS在预测止血干预需求方面比GBS更准确(接受者工作曲线下面积(AUROC) 0.82;95% CI 0.78 ~ 0.86 vs 0.72;95% CI 0.67 ~ 0.77;结论:LHS在预测AUGIB患者是否需要止血干预方面是准确的,并可用于识别一定比例的低风险患者,这些患者可以接受延迟或门诊内镜检查。在常规临床使用之前,需要在其他地理环境中进行验证。
Derivation and validation of a novel risk score to predict need for haemostatic intervention in acute upper gastrointestinal bleeding (London Haemostat Score).
Background: Acute upper gastrointestinal bleeding (AUGIB) is a common medical emergency, which takes up considerable healthcare resources. However, only approximately 20%-30% of bleeds require urgent haemostatic intervention. Current standard of care is for all patients admitted to hospital to undergo endoscopy within 24 hours for risk stratification, but this is difficult to achieve in practice, invasive and costly.
Aim: To develop a novel non-endoscopic risk stratification tool for AUGIB to predict the need for haemostatic intervention by endoscopic, radiological or surgical treatments. We compared this with the Glasgow-Blatchford Score (GBS).
Design: Model development was carried out using a derivation (n=466) and prospectively collected validation cohort (n=404) of patients who were admitted with AUGIB to three large hospitals in London, UK (2015-2020). Univariable and multivariable logistic regression analysis was used to identify variables that were associated with increased or decreased chances of requiring haemostatic intervention. This model was converted into a risk scoring system, the London Haemostat Score (LHS).
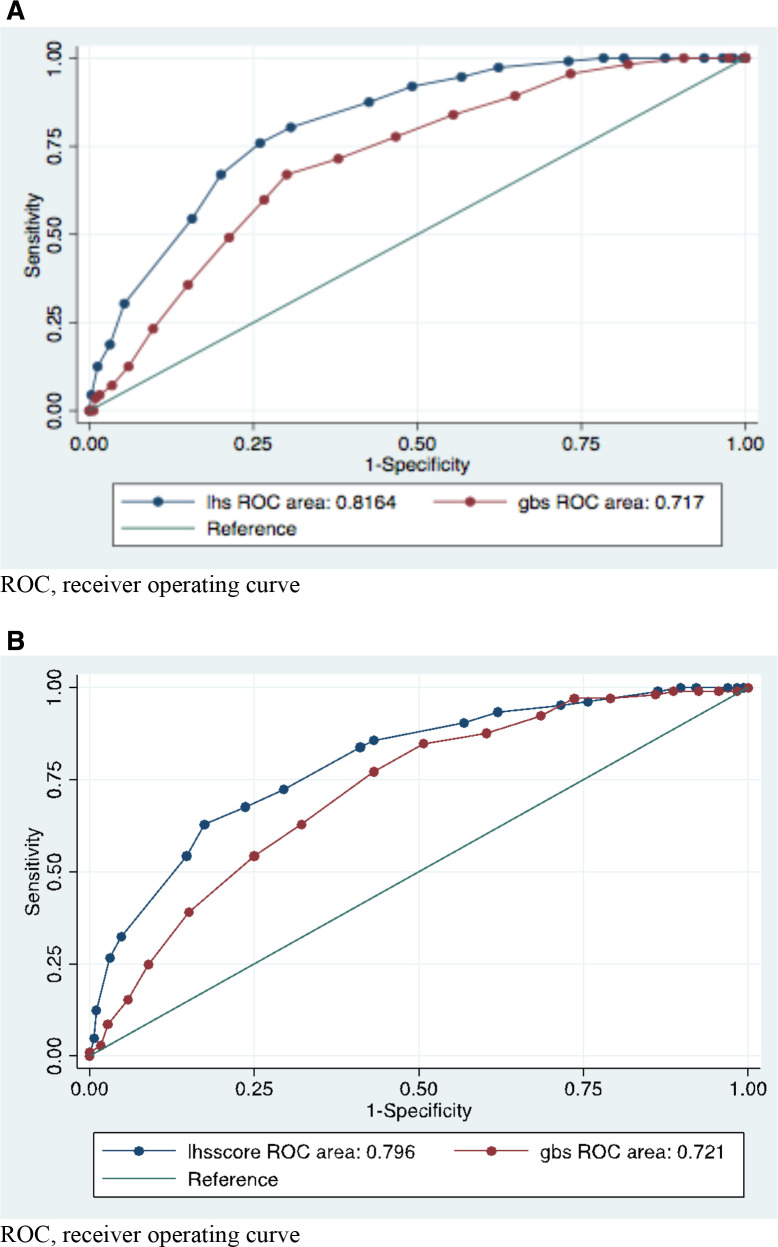
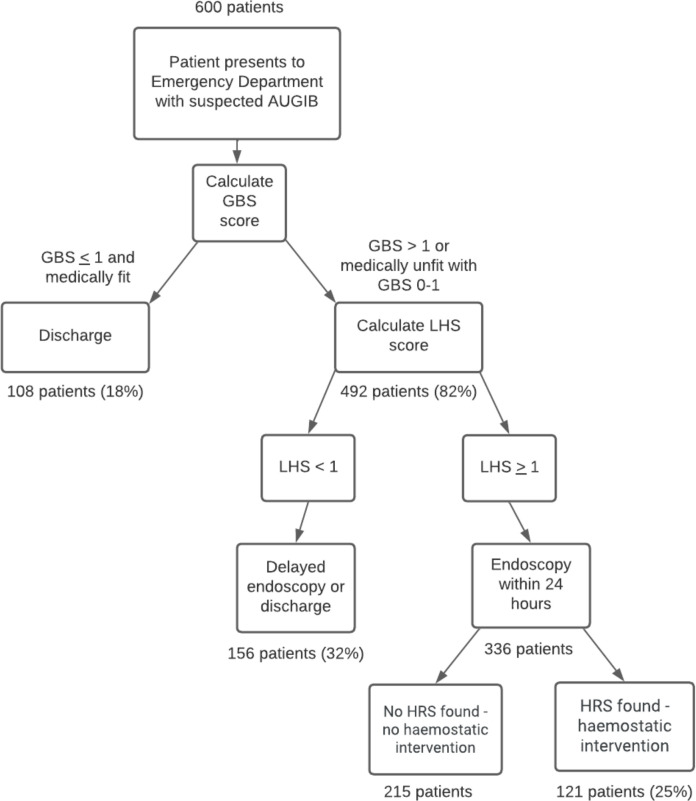
Results: The LHS was more accurate at predicting need for haemostatic intervention than the GBS, in the derivation cohort (area under the receiver operating curve (AUROC) 0.82; 95% CI 0.78 to 0.86 vs 0.72; 95% CI 0.67 to 0.77; p<0.001) and validation cohort (AUROC 0.80; 95% CI 0.75 to 0.85 vs 0.72; 95% CI 0.67 to 0.78; p<0.001). At cut-off scores at which LHS and GBS identified patients who required haemostatic intervention with 98% sensitivity, the specificity of the LHS was 41% vs 18% with the GBS (p<0.001). This could translate to 32% of inpatient endoscopies for AUGIB being avoided at a cost of only a 0.5% false negative rate.
Conclusions: The LHS is accurate at predicting the need for haemostatic intervention in AUGIB and could be used to identify a proportion of low-risk patients who can undergo delayed or outpatient endoscopy. Validation in other geographical settings is required before routine clinical use.
期刊介绍:
BMJ Open Gastroenterology is an online-only, peer-reviewed, open access gastroenterology journal, dedicated to publishing high-quality medical research from all disciplines and therapeutic areas of gastroenterology. It is the open access companion journal of Gut and is co-owned by the British Society of Gastroenterology. The journal publishes all research study types, from study protocols to phase I trials to meta-analyses, including small or specialist studies. Publishing procedures are built around continuous publication, publishing research online as soon as the article is ready.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


