Patrick M Chen, Sophie Schuurmans Stekhoven, Adnan Haider, Jin Jing, Wendong Ge, Eric S Rosenthal, M Brandon Westover, Sahar F Zafar
{"title":"癫痫样活动与毒性代谢性脑病预后的关系。","authors":"Patrick M Chen, Sophie Schuurmans Stekhoven, Adnan Haider, Jin Jing, Wendong Ge, Eric S Rosenthal, M Brandon Westover, Sahar F Zafar","doi":"10.1097/CCE.0000000000000913","DOIUrl":null,"url":null,"abstract":"<p><p>The clinical significance of epileptiform abnormalities (EAs) specific to toxic-metabolic encephalopathy (TME) is unknown.</p><p><strong>Objectives: </strong>To quantify EA burden in patients with TME and its association with neurologic outcomes.</p><p><strong>Design setting and participant: </strong>This is a retrospective study. A cohort of patients with TME and EA (positive) were age, Sequential Organ Failure Assessment Score, Acute Physiology and Chronic Health Evaluation II (APACHE-II) score matched to a cohort of TME patients without EA (control). Univariate analysis compared EA-positive patients against controls. Multivariable logistical regression adjusting for underlying disease etiology was performed to examine the relationship between EA burden and probability of poor neurologic outcome (modified Rankin Score [mRS] 4-6) at discharge. Consecutive admissions to inpatient floors or ICUs that underwent continuous electroencephalography (cEEG) monitoring at a single center between 2012 and 2019. Inclusion criteria were 1) patients with TME diagnosis, 2) age greater than 18 years, and 3) greater than or equal to 16 hours of cEEG. Patients with acute brain injury and cardiac arrest were excluded.</p><p><strong>Main outcomes and measures: </strong>Poor neurologic outcome defined by mRS (mRS 4-6).</p><p><strong>Results: </strong>One hundred sixteen patients were included, 58 with EA and 58 controls without EA, where matching was performed on age and APACHE-II score. The median age was 66 (Q1-Q3, 57-75) and median APACHE II score was 18 (Q1-Q3, 13-22). Overall cohort discharge mortality was 22% and 70% had a poor neurologic outcome. Peak EA burden was defined as the 12-hour window of recording with the highest prevalence of EAs. In multivariable analysis adjusted for Charlson Comorbidity Index and primary diagnosis, presence of EAs was associated with poor outcome (odds ratio 3.89; CI [1.05-14.2], <i>p</i> = 0.041). Increase in peak EA burden from 0% to 100% increased probability of poor discharge neurologic outcome by 30%.</p><p><strong>Conclusions and relevance: </strong>Increasing burden of EA is associated with worse discharge outcomes in patients with TME. Future studies are needed to determine whether short-term treatment with anti-seizure medications while medically treating the underlying metabolic derangement improves outcomes.</p>","PeriodicalId":10759,"journal":{"name":"Critical Care Explorations","volume":"5 5","pages":"e0913"},"PeriodicalIF":0.0000,"publicationDate":"2023-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5d/da/cc9-5-e0913.PMC10166342.pdf","citationCount":"0","resultStr":"{\"title\":\"Association of Epileptiform Activity With Outcomes in Toxic-Metabolic Encephalopathy.\",\"authors\":\"Patrick M Chen, Sophie Schuurmans Stekhoven, Adnan Haider, Jin Jing, Wendong Ge, Eric S Rosenthal, M Brandon Westover, Sahar F Zafar\",\"doi\":\"10.1097/CCE.0000000000000913\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The clinical significance of epileptiform abnormalities (EAs) specific to toxic-metabolic encephalopathy (TME) is unknown.</p><p><strong>Objectives: </strong>To quantify EA burden in patients with TME and its association with neurologic outcomes.</p><p><strong>Design setting and participant: </strong>This is a retrospective study. A cohort of patients with TME and EA (positive) were age, Sequential Organ Failure Assessment Score, Acute Physiology and Chronic Health Evaluation II (APACHE-II) score matched to a cohort of TME patients without EA (control). Univariate analysis compared EA-positive patients against controls. Multivariable logistical regression adjusting for underlying disease etiology was performed to examine the relationship between EA burden and probability of poor neurologic outcome (modified Rankin Score [mRS] 4-6) at discharge. Consecutive admissions to inpatient floors or ICUs that underwent continuous electroencephalography (cEEG) monitoring at a single center between 2012 and 2019. Inclusion criteria were 1) patients with TME diagnosis, 2) age greater than 18 years, and 3) greater than or equal to 16 hours of cEEG. Patients with acute brain injury and cardiac arrest were excluded.</p><p><strong>Main outcomes and measures: </strong>Poor neurologic outcome defined by mRS (mRS 4-6).</p><p><strong>Results: </strong>One hundred sixteen patients were included, 58 with EA and 58 controls without EA, where matching was performed on age and APACHE-II score. The median age was 66 (Q1-Q3, 57-75) and median APACHE II score was 18 (Q1-Q3, 13-22). Overall cohort discharge mortality was 22% and 70% had a poor neurologic outcome. Peak EA burden was defined as the 12-hour window of recording with the highest prevalence of EAs. In multivariable analysis adjusted for Charlson Comorbidity Index and primary diagnosis, presence of EAs was associated with poor outcome (odds ratio 3.89; CI [1.05-14.2], <i>p</i> = 0.041). Increase in peak EA burden from 0% to 100% increased probability of poor discharge neurologic outcome by 30%.</p><p><strong>Conclusions and relevance: </strong>Increasing burden of EA is associated with worse discharge outcomes in patients with TME. Future studies are needed to determine whether short-term treatment with anti-seizure medications while medically treating the underlying metabolic derangement improves outcomes.</p>\",\"PeriodicalId\":10759,\"journal\":{\"name\":\"Critical Care Explorations\",\"volume\":\"5 5\",\"pages\":\"e0913\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5d/da/cc9-5-e0913.PMC10166342.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Care Explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000000913\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000000913","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Association of Epileptiform Activity With Outcomes in Toxic-Metabolic Encephalopathy.
The clinical significance of epileptiform abnormalities (EAs) specific to toxic-metabolic encephalopathy (TME) is unknown.
Objectives: To quantify EA burden in patients with TME and its association with neurologic outcomes.
Design setting and participant: This is a retrospective study. A cohort of patients with TME and EA (positive) were age, Sequential Organ Failure Assessment Score, Acute Physiology and Chronic Health Evaluation II (APACHE-II) score matched to a cohort of TME patients without EA (control). Univariate analysis compared EA-positive patients against controls. Multivariable logistical regression adjusting for underlying disease etiology was performed to examine the relationship between EA burden and probability of poor neurologic outcome (modified Rankin Score [mRS] 4-6) at discharge. Consecutive admissions to inpatient floors or ICUs that underwent continuous electroencephalography (cEEG) monitoring at a single center between 2012 and 2019. Inclusion criteria were 1) patients with TME diagnosis, 2) age greater than 18 years, and 3) greater than or equal to 16 hours of cEEG. Patients with acute brain injury and cardiac arrest were excluded.
Main outcomes and measures: Poor neurologic outcome defined by mRS (mRS 4-6).
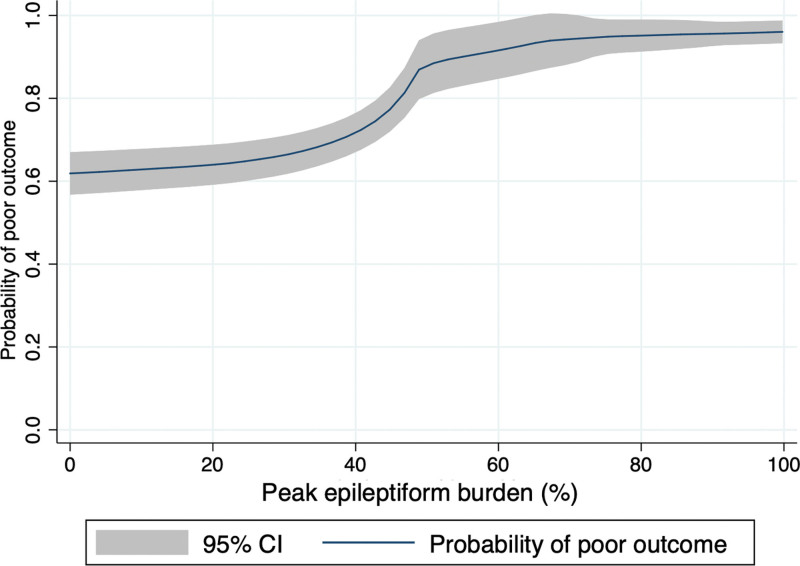
Results: One hundred sixteen patients were included, 58 with EA and 58 controls without EA, where matching was performed on age and APACHE-II score. The median age was 66 (Q1-Q3, 57-75) and median APACHE II score was 18 (Q1-Q3, 13-22). Overall cohort discharge mortality was 22% and 70% had a poor neurologic outcome. Peak EA burden was defined as the 12-hour window of recording with the highest prevalence of EAs. In multivariable analysis adjusted for Charlson Comorbidity Index and primary diagnosis, presence of EAs was associated with poor outcome (odds ratio 3.89; CI [1.05-14.2], p = 0.041). Increase in peak EA burden from 0% to 100% increased probability of poor discharge neurologic outcome by 30%.
Conclusions and relevance: Increasing burden of EA is associated with worse discharge outcomes in patients with TME. Future studies are needed to determine whether short-term treatment with anti-seizure medications while medically treating the underlying metabolic derangement improves outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


