Catherine Le Berre, Silvio Danese, Laurent Peyrin-Biroulet
{"title":"我们能改变炎症性肠病的自然病程吗?","authors":"Catherine Le Berre, Silvio Danese, Laurent Peyrin-Biroulet","doi":"10.1177/17562848231163118","DOIUrl":null,"url":null,"abstract":"<p><p>Inflammatory bowel diseases (IBD), including Crohn's disease (CD) and ulcerative colitis (UC), are lifelong diseases characterized by chronic inflammation of the gastrointestinal tract leading to its progressive and irreversible destruction. Whether early initiation of IBD-specific therapy impacts the long-term course of the disease remains unclear and has to be further explored in prospective disease-modification trials. Historically, surgery and hospitalization rates have been the surrogate markers to measure disease progression in IBD, providing an overview of the effectiveness of medical therapies. However, neither surgery nor hospitalization necessarily reflects a fail in therapeutic medical management, and many confounding factors make them biased outcomes. The Selecting Endpoints for Disease-Modification Trials consensus has defined the disease-modification endpoints required for these trials, including the impact of the disease on patient's life (health-related quality of life, disability, and fecal incontinence), the mid-term disease complications (bowel damage in CD, IBD-related surgery and hospitalizations, disease extension in UC, extra-intestinal manifestations, permanent stoma, short bowel syndrome), and the development of dysplasia/cancer and mortality in the long term. Most available data in the literature regarding the impact of current therapies on disease progression focused on anti-tumor necrosis factor agents and are based on retrospective or post-hoc studies. Thus, prospective disease-modification trials are pressingly required to explore the effectiveness of early intensified treatment in patients with severe disease or at risk for disease progression.</p>","PeriodicalId":23022,"journal":{"name":"Therapeutic Advances in Gastroenterology","volume":"16 ","pages":"17562848231163118"},"PeriodicalIF":3.4000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f0/19/10.1177_17562848231163118.PMC10159495.pdf","citationCount":"1","resultStr":"{\"title\":\"Can we change the natural course of inflammatory bowel disease?\",\"authors\":\"Catherine Le Berre, Silvio Danese, Laurent Peyrin-Biroulet\",\"doi\":\"10.1177/17562848231163118\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Inflammatory bowel diseases (IBD), including Crohn's disease (CD) and ulcerative colitis (UC), are lifelong diseases characterized by chronic inflammation of the gastrointestinal tract leading to its progressive and irreversible destruction. Whether early initiation of IBD-specific therapy impacts the long-term course of the disease remains unclear and has to be further explored in prospective disease-modification trials. Historically, surgery and hospitalization rates have been the surrogate markers to measure disease progression in IBD, providing an overview of the effectiveness of medical therapies. However, neither surgery nor hospitalization necessarily reflects a fail in therapeutic medical management, and many confounding factors make them biased outcomes. The Selecting Endpoints for Disease-Modification Trials consensus has defined the disease-modification endpoints required for these trials, including the impact of the disease on patient's life (health-related quality of life, disability, and fecal incontinence), the mid-term disease complications (bowel damage in CD, IBD-related surgery and hospitalizations, disease extension in UC, extra-intestinal manifestations, permanent stoma, short bowel syndrome), and the development of dysplasia/cancer and mortality in the long term. Most available data in the literature regarding the impact of current therapies on disease progression focused on anti-tumor necrosis factor agents and are based on retrospective or post-hoc studies. Thus, prospective disease-modification trials are pressingly required to explore the effectiveness of early intensified treatment in patients with severe disease or at risk for disease progression.</p>\",\"PeriodicalId\":23022,\"journal\":{\"name\":\"Therapeutic Advances in Gastroenterology\",\"volume\":\"16 \",\"pages\":\"17562848231163118\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f0/19/10.1177_17562848231163118.PMC10159495.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Gastroenterology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/17562848231163118\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562848231163118","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Can we change the natural course of inflammatory bowel disease?
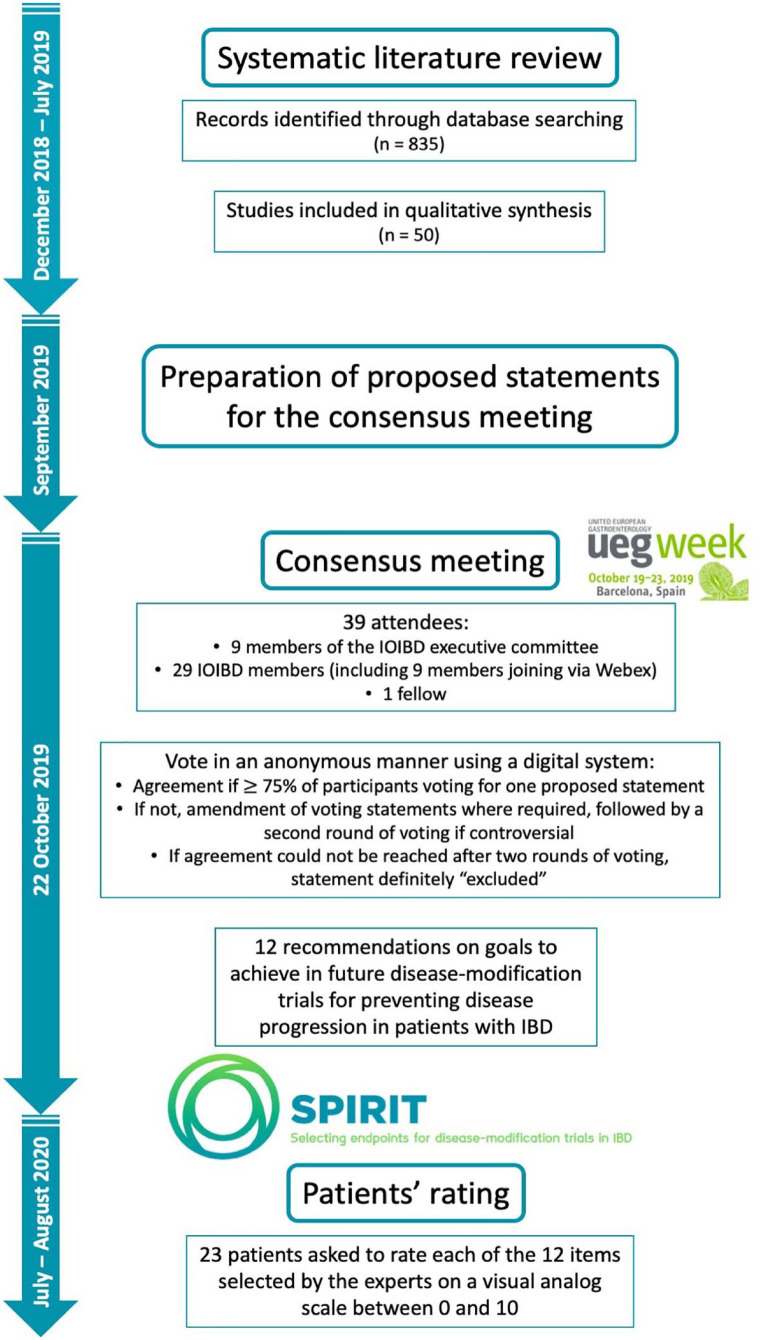
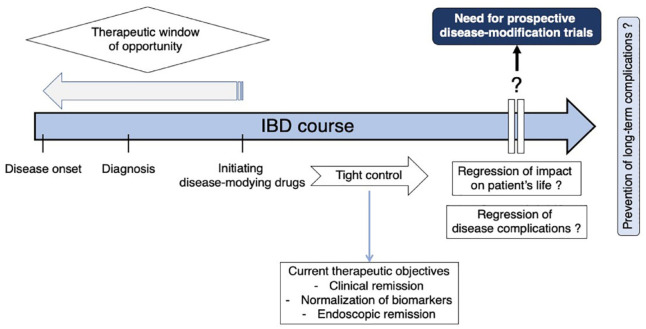
Inflammatory bowel diseases (IBD), including Crohn's disease (CD) and ulcerative colitis (UC), are lifelong diseases characterized by chronic inflammation of the gastrointestinal tract leading to its progressive and irreversible destruction. Whether early initiation of IBD-specific therapy impacts the long-term course of the disease remains unclear and has to be further explored in prospective disease-modification trials. Historically, surgery and hospitalization rates have been the surrogate markers to measure disease progression in IBD, providing an overview of the effectiveness of medical therapies. However, neither surgery nor hospitalization necessarily reflects a fail in therapeutic medical management, and many confounding factors make them biased outcomes. The Selecting Endpoints for Disease-Modification Trials consensus has defined the disease-modification endpoints required for these trials, including the impact of the disease on patient's life (health-related quality of life, disability, and fecal incontinence), the mid-term disease complications (bowel damage in CD, IBD-related surgery and hospitalizations, disease extension in UC, extra-intestinal manifestations, permanent stoma, short bowel syndrome), and the development of dysplasia/cancer and mortality in the long term. Most available data in the literature regarding the impact of current therapies on disease progression focused on anti-tumor necrosis factor agents and are based on retrospective or post-hoc studies. Thus, prospective disease-modification trials are pressingly required to explore the effectiveness of early intensified treatment in patients with severe disease or at risk for disease progression.
期刊介绍:
Therapeutic Advances in Gastroenterology is an open access journal which delivers the highest quality peer-reviewed original research articles, reviews, and scholarly comment on pioneering efforts and innovative studies in the medical treatment of gastrointestinal and hepatic disorders. The journal has a strong clinical and pharmacological focus and is aimed at an international audience of clinicians and researchers in gastroenterology and related disciplines, providing an online forum for rapid dissemination of recent research and perspectives in this area.
The editors welcome original research articles across all areas of gastroenterology and hepatology.
The journal publishes original research articles and review articles primarily. Original research manuscripts may include laboratory, animal or human/clinical studies – all phases. Letters to the Editor and Case Reports will also be considered.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


