Paul Geenty, Shanthosh Sivapathan, Luke D Stefani, Matthew Zada, Anita Boyd, David Richards, Fiona Kwok, Liza Thomas
{"title":"一种新的轻链淀粉样变性超声心动图风险评分方法。","authors":"Paul Geenty, Shanthosh Sivapathan, Luke D Stefani, Matthew Zada, Anita Boyd, David Richards, Fiona Kwok, Liza Thomas","doi":"10.1093/ehjopen/oead040","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The prognosis of light-chain (AL) amyloidosis, a plasma cell dyscrasia, is largely determined by the presence of cardiac involvement. Conventional staging is achieved using cardiac biomarkers (high-sensitivity troponin, <i>N</i>-terminal pro-beta natriuretic peptide) and free light-chain difference (Mayo staging). We sought to evaluate the role of echocardiographic parameters as prognostic markers in AL amyloidosis and examine their utility compared with conventional staging.</p><p><strong>Methods and results: </strong>Seventy-five consecutive patients with AL amyloidosis reviewed at a referral amyloid clinic who underwent comprehensive echocardiographic assessment were retrospectively identified. The evaluated echocardiographic parameters included left ventricular (LV) ejection fraction, mass, diastolic function parameters, global longitudinal strain (GLS), and left atrial (LA) volume. Mortality was assessed through a review of clinical records. During a median follow-up of 51 months, 29/75 (39%) patients died. Patients who died had a larger LA volume (47 ± 12 vs. 35 ± 10 mL/m<sup>2</sup>, <i>P</i> < 0.001) and a higher <i>E</i>/<i>e</i>' (18 ± 10 vs. 14 ± 6, <i>P</i> = 0.026). Univariate clinical and echocardiographic predictors of survival included LA volume, <i>E</i>/<i>e</i>', <i>e</i>', LVGLS, and Mayo stage (at significance of <i>P</i> < 0.1). Left atrial volume and LVGLS were significant determinants of mortality when examined using clinical cut-offs, although <i>E</i>/<i>e</i>' was not. A composite echocardiographic risk score comprising LA volume and LVGLS provided similar prognostic performance to Mayo stage [area under the curve (AUC) 0.75, 95% confidence interval (CI) 0.64-0.85 vs. AUC 0.75, 95% CI 0.65-0.858, <i>P</i> = 0.91].</p><p><strong>Conclusion: </strong>Left atrial volume and LVGLS were independent predictors of mortality in AL amyloidosis. A composite echocardiographic score combining LA volume and LVGLS has similar prognostic power to Mayo stage for all-cause mortality.</p>","PeriodicalId":11973,"journal":{"name":"European Heart Journal Open","volume":"3 3","pages":"oead040"},"PeriodicalIF":0.0000,"publicationDate":"2023-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a4/e6/oead040.PMC10152390.pdf","citationCount":"1","resultStr":"{\"title\":\"A novel echocardiographic risk score for light-chain amyloidosis.\",\"authors\":\"Paul Geenty, Shanthosh Sivapathan, Luke D Stefani, Matthew Zada, Anita Boyd, David Richards, Fiona Kwok, Liza Thomas\",\"doi\":\"10.1093/ehjopen/oead040\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>The prognosis of light-chain (AL) amyloidosis, a plasma cell dyscrasia, is largely determined by the presence of cardiac involvement. Conventional staging is achieved using cardiac biomarkers (high-sensitivity troponin, <i>N</i>-terminal pro-beta natriuretic peptide) and free light-chain difference (Mayo staging). We sought to evaluate the role of echocardiographic parameters as prognostic markers in AL amyloidosis and examine their utility compared with conventional staging.</p><p><strong>Methods and results: </strong>Seventy-five consecutive patients with AL amyloidosis reviewed at a referral amyloid clinic who underwent comprehensive echocardiographic assessment were retrospectively identified. The evaluated echocardiographic parameters included left ventricular (LV) ejection fraction, mass, diastolic function parameters, global longitudinal strain (GLS), and left atrial (LA) volume. Mortality was assessed through a review of clinical records. During a median follow-up of 51 months, 29/75 (39%) patients died. Patients who died had a larger LA volume (47 ± 12 vs. 35 ± 10 mL/m<sup>2</sup>, <i>P</i> < 0.001) and a higher <i>E</i>/<i>e</i>' (18 ± 10 vs. 14 ± 6, <i>P</i> = 0.026). Univariate clinical and echocardiographic predictors of survival included LA volume, <i>E</i>/<i>e</i>', <i>e</i>', LVGLS, and Mayo stage (at significance of <i>P</i> < 0.1). Left atrial volume and LVGLS were significant determinants of mortality when examined using clinical cut-offs, although <i>E</i>/<i>e</i>' was not. A composite echocardiographic risk score comprising LA volume and LVGLS provided similar prognostic performance to Mayo stage [area under the curve (AUC) 0.75, 95% confidence interval (CI) 0.64-0.85 vs. AUC 0.75, 95% CI 0.65-0.858, <i>P</i> = 0.91].</p><p><strong>Conclusion: </strong>Left atrial volume and LVGLS were independent predictors of mortality in AL amyloidosis. A composite echocardiographic score combining LA volume and LVGLS has similar prognostic power to Mayo stage for all-cause mortality.</p>\",\"PeriodicalId\":11973,\"journal\":{\"name\":\"European Heart Journal Open\",\"volume\":\"3 3\",\"pages\":\"oead040\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a4/e6/oead040.PMC10152390.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Heart Journal Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjopen/oead040\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oead040","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
摘要
目的:轻链(AL)淀粉样变性是一种浆细胞病变,其预后在很大程度上取决于是否累及心脏。传统的分期是通过心脏生物标志物(高灵敏度肌钙蛋白、n端前-利钠肽)和游离轻链差异(梅奥分期)来实现的。我们试图评估超声心动图参数作为AL淀粉样变的预后标志物的作用,并将其与常规分期进行比较。方法和结果:回顾性分析了在淀粉样蛋白转诊诊所接受全面超声心动图评估的75例连续AL淀粉样变性患者。评估的超声心动图参数包括左室(LV)射血分数、质量、舒张功能参数、总纵应变(GLS)和左心房(LA)容积。通过对临床记录的回顾来评估死亡率。在51个月的中位随访期间,29/75(39%)患者死亡。死亡患者LA容积较大(47±12 vs 35±10 mL/m2, P < 0.001), E/ E′较高(18±10 vs 14±6,P = 0.026)。单因素临床和超声心动图预后指标包括LA容积、E/ E′、E′、LVGLS和Mayo分期(P < 0.1)。当使用临床临界值检查时,左房容积和左室gls是死亡率的重要决定因素,尽管E/ E '不是。由LA容积和LVGLS组成的复合超声心动图风险评分提供了与Mayo分期相似的预后表现[曲线下面积(AUC) 0.75, 95%置信区间(CI) 0.64-0.85 vs. AUC 0.75, 95% CI 0.65-0.858, P = 0.91]。结论:左房容积和左室gls是AL淀粉样变性患者死亡率的独立预测因子。结合左室容积和左室gls的复合超声心动图评分对于全因死亡率具有与Mayo分期相似的预后能力。
A novel echocardiographic risk score for light-chain amyloidosis.
Aims: The prognosis of light-chain (AL) amyloidosis, a plasma cell dyscrasia, is largely determined by the presence of cardiac involvement. Conventional staging is achieved using cardiac biomarkers (high-sensitivity troponin, N-terminal pro-beta natriuretic peptide) and free light-chain difference (Mayo staging). We sought to evaluate the role of echocardiographic parameters as prognostic markers in AL amyloidosis and examine their utility compared with conventional staging.
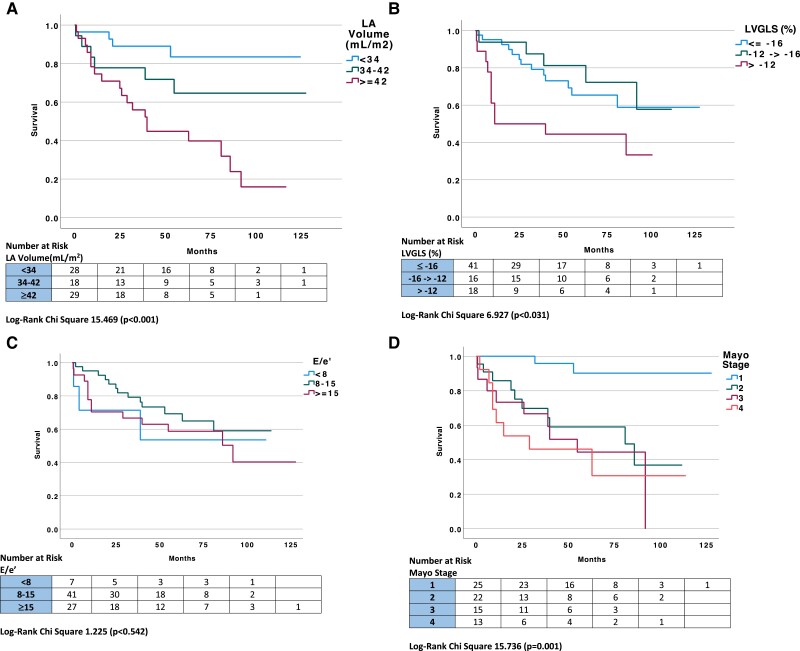
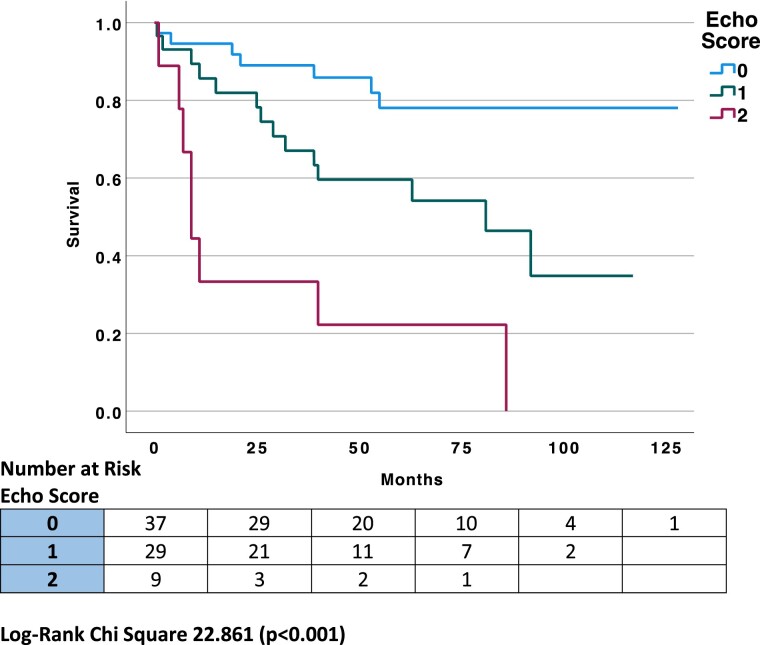
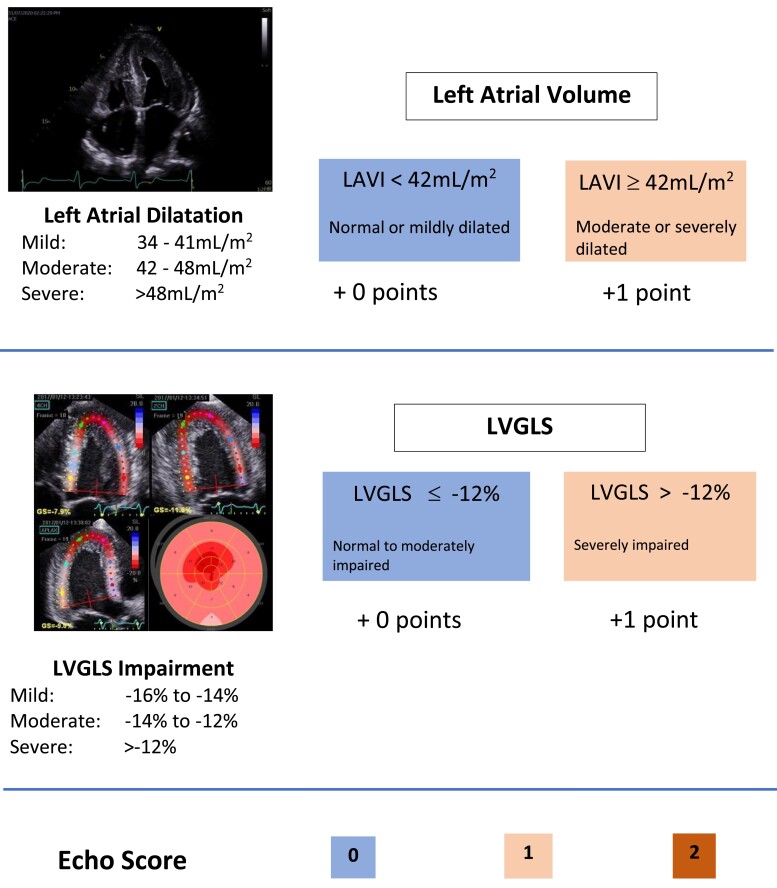
Methods and results: Seventy-five consecutive patients with AL amyloidosis reviewed at a referral amyloid clinic who underwent comprehensive echocardiographic assessment were retrospectively identified. The evaluated echocardiographic parameters included left ventricular (LV) ejection fraction, mass, diastolic function parameters, global longitudinal strain (GLS), and left atrial (LA) volume. Mortality was assessed through a review of clinical records. During a median follow-up of 51 months, 29/75 (39%) patients died. Patients who died had a larger LA volume (47 ± 12 vs. 35 ± 10 mL/m2, P < 0.001) and a higher E/e' (18 ± 10 vs. 14 ± 6, P = 0.026). Univariate clinical and echocardiographic predictors of survival included LA volume, E/e', e', LVGLS, and Mayo stage (at significance of P < 0.1). Left atrial volume and LVGLS were significant determinants of mortality when examined using clinical cut-offs, although E/e' was not. A composite echocardiographic risk score comprising LA volume and LVGLS provided similar prognostic performance to Mayo stage [area under the curve (AUC) 0.75, 95% confidence interval (CI) 0.64-0.85 vs. AUC 0.75, 95% CI 0.65-0.858, P = 0.91].
Conclusion: Left atrial volume and LVGLS were independent predictors of mortality in AL amyloidosis. A composite echocardiographic score combining LA volume and LVGLS has similar prognostic power to Mayo stage for all-cause mortality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


