Meng Wang, Feifan Zhao, Lina Sun, Ying Liang, Wei Yan, Xiaoyan Sun, Qingtao Zhou, Bei He
{"title":"呼吸性酸中毒 AECOPD 患者的高流量鼻导管与无创通气:倾向评分匹配的回顾性研究。","authors":"Meng Wang, Feifan Zhao, Lina Sun, Ying Liang, Wei Yan, Xiaoyan Sun, Qingtao Zhou, Bei He","doi":"10.1155/2023/6377441","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Limited data are available about the clinical outcomes of AECOPD patients with respiratory acidosis treated with HFNC versus NIV.</p><p><strong>Methods: </strong>We conducted a retrospective study to compare the efficacy of HFNC with NIV as initial ventilation support strategy in AECOPD patients with respiratory acidosis. Propensity score matching (PSM) was implemented to increase between-group comparability. Kaplan-Meier analysis was utilized to evaluate differences between the HFNC success, HFNC failure, and NIV groups. Univariate analysis was performed to identify the features that differed significantly between the HFNC success and HFNC failure groups.</p><p><strong>Results: </strong>After screening 2219 hospitalization records, 44 patients from the HFNC group and 44 from the NIV group were successfully matched after PSM. The 30-day mortality (4.5% versus 6.8%, <i>p</i> = 0.645) and 90-day mortality (4.5% versus 11.4%, <i>p</i> = 0.237) did not differ between the HFNC and NIV groups. Length of ICU stay (median: 11 versus 18 days, <i>p</i> = 0.001), length of hospital stay (median: 14 versus 20 days, <i>p</i> = 0.001), and hospital cost (median: 4392 versus 8403 $USD, <i>p</i> = 0.001) were significantly lower in the HFNC group compared with NIV group. The treatment failure rate was much higher in the HFNC group than in the NIV group (38.6% versus 11.4%, <i>p</i> = 0.003). However, patients who experienced HFNC failure and switched to NIV showed similar clinical outcomes to those who first received NIV. Univariate analysis showed that log NT-proBNP was an important factor for HFNC failure (<i>p</i> = 0.007).</p><p><strong>Conclusions: </strong>Compared with NIV, HFNC followed by NIV as rescue therapy may be a viable initial ventilation support strategy for AECOPD patients with respiratory acidosis. NT-proBNP may be an important factor for HFNC failure in these patients. Further well-designed randomized controlled trials are needed for more accurate and reliable results.</p>","PeriodicalId":9416,"journal":{"name":"Canadian respiratory journal","volume":"2023 ","pages":"6377441"},"PeriodicalIF":2.1000,"publicationDate":"2023-04-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10122591/pdf/","citationCount":"0","resultStr":"{\"title\":\"High-Flow Nasal Cannula versus Noninvasive Ventilation in AECOPD Patients with Respiratory Acidosis: A Retrospective Propensity Score-Matched Study.\",\"authors\":\"Meng Wang, Feifan Zhao, Lina Sun, Ying Liang, Wei Yan, Xiaoyan Sun, Qingtao Zhou, Bei He\",\"doi\":\"10.1155/2023/6377441\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Limited data are available about the clinical outcomes of AECOPD patients with respiratory acidosis treated with HFNC versus NIV.</p><p><strong>Methods: </strong>We conducted a retrospective study to compare the efficacy of HFNC with NIV as initial ventilation support strategy in AECOPD patients with respiratory acidosis. Propensity score matching (PSM) was implemented to increase between-group comparability. Kaplan-Meier analysis was utilized to evaluate differences between the HFNC success, HFNC failure, and NIV groups. Univariate analysis was performed to identify the features that differed significantly between the HFNC success and HFNC failure groups.</p><p><strong>Results: </strong>After screening 2219 hospitalization records, 44 patients from the HFNC group and 44 from the NIV group were successfully matched after PSM. The 30-day mortality (4.5% versus 6.8%, <i>p</i> = 0.645) and 90-day mortality (4.5% versus 11.4%, <i>p</i> = 0.237) did not differ between the HFNC and NIV groups. Length of ICU stay (median: 11 versus 18 days, <i>p</i> = 0.001), length of hospital stay (median: 14 versus 20 days, <i>p</i> = 0.001), and hospital cost (median: 4392 versus 8403 $USD, <i>p</i> = 0.001) were significantly lower in the HFNC group compared with NIV group. The treatment failure rate was much higher in the HFNC group than in the NIV group (38.6% versus 11.4%, <i>p</i> = 0.003). However, patients who experienced HFNC failure and switched to NIV showed similar clinical outcomes to those who first received NIV. Univariate analysis showed that log NT-proBNP was an important factor for HFNC failure (<i>p</i> = 0.007).</p><p><strong>Conclusions: </strong>Compared with NIV, HFNC followed by NIV as rescue therapy may be a viable initial ventilation support strategy for AECOPD patients with respiratory acidosis. NT-proBNP may be an important factor for HFNC failure in these patients. Further well-designed randomized controlled trials are needed for more accurate and reliable results.</p>\",\"PeriodicalId\":9416,\"journal\":{\"name\":\"Canadian respiratory journal\",\"volume\":\"2023 \",\"pages\":\"6377441\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2023-04-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10122591/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canadian respiratory journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1155/2023/6377441\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian respiratory journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2023/6377441","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
High-Flow Nasal Cannula versus Noninvasive Ventilation in AECOPD Patients with Respiratory Acidosis: A Retrospective Propensity Score-Matched Study.
Background: Limited data are available about the clinical outcomes of AECOPD patients with respiratory acidosis treated with HFNC versus NIV.
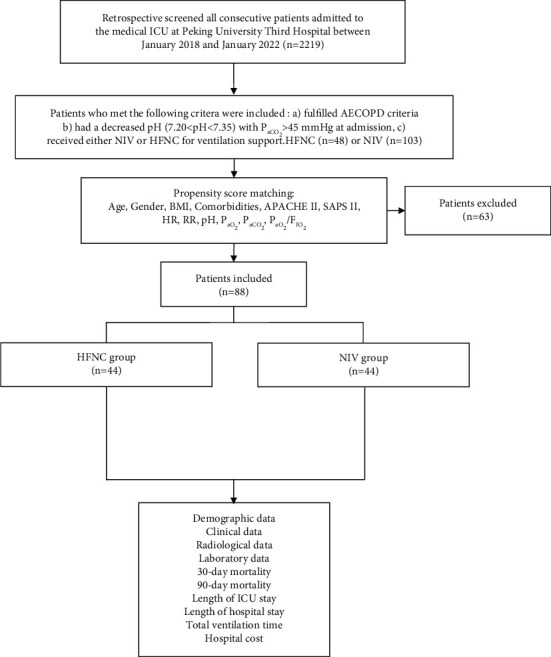
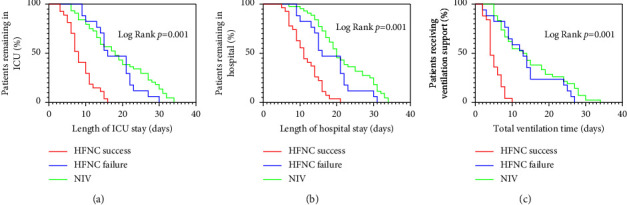
Methods: We conducted a retrospective study to compare the efficacy of HFNC with NIV as initial ventilation support strategy in AECOPD patients with respiratory acidosis. Propensity score matching (PSM) was implemented to increase between-group comparability. Kaplan-Meier analysis was utilized to evaluate differences between the HFNC success, HFNC failure, and NIV groups. Univariate analysis was performed to identify the features that differed significantly between the HFNC success and HFNC failure groups.
Results: After screening 2219 hospitalization records, 44 patients from the HFNC group and 44 from the NIV group were successfully matched after PSM. The 30-day mortality (4.5% versus 6.8%, p = 0.645) and 90-day mortality (4.5% versus 11.4%, p = 0.237) did not differ between the HFNC and NIV groups. Length of ICU stay (median: 11 versus 18 days, p = 0.001), length of hospital stay (median: 14 versus 20 days, p = 0.001), and hospital cost (median: 4392 versus 8403 $USD, p = 0.001) were significantly lower in the HFNC group compared with NIV group. The treatment failure rate was much higher in the HFNC group than in the NIV group (38.6% versus 11.4%, p = 0.003). However, patients who experienced HFNC failure and switched to NIV showed similar clinical outcomes to those who first received NIV. Univariate analysis showed that log NT-proBNP was an important factor for HFNC failure (p = 0.007).
Conclusions: Compared with NIV, HFNC followed by NIV as rescue therapy may be a viable initial ventilation support strategy for AECOPD patients with respiratory acidosis. NT-proBNP may be an important factor for HFNC failure in these patients. Further well-designed randomized controlled trials are needed for more accurate and reliable results.
期刊介绍:
Canadian Respiratory Journal is a peer-reviewed, Open Access journal that aims to provide a multidisciplinary forum for research in all areas of respiratory medicine. The journal publishes original research articles, review articles, and clinical studies related to asthma, allergy, COPD, non-invasive ventilation, therapeutic intervention, lung cancer, airway and lung infections, as well as any other respiratory diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


