Anthony F Yu, Chau T Dang, Justine Jorgensen, Chaya S Moskowitz, Patricia DeFusco, Eric Oligino, Kevin C Oeffinger, Jennifer E Liu, Richard M Steingart
{"title":"在her2靶向治疗期间减少心脏毒性监测的心脏安全性研究的基本原理和设计。","authors":"Anthony F Yu, Chau T Dang, Justine Jorgensen, Chaya S Moskowitz, Patricia DeFusco, Eric Oligino, Kevin C Oeffinger, Jennifer E Liu, Richard M Steingart","doi":"10.1186/s40959-023-00163-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Echocardiograms are recommended every 3 months in patients receiving human epidermal growth factor 2 (HER2)-targeted therapy for surveillance of left ventricular ejection fraction (LVEF). Efforts to tailor treatment for HER2-positive breast cancer have led to greater use of non-anthracycline regimens that are associated with lower cardiotoxicity risk, raising into question the need for frequent cardiotoxicity surveillance for these patients. This study seeks to evaluate whether less frequent cardiotoxicity surveillance (every 6 months) is safe for patients receiving a non-anthracycline HER2-targeted treatment regimen.</p><p><strong>Methods/design: </strong>We will enroll 190 women with histologically confirmed HER2-positive breast cancer scheduled to receive a non-anthracycline HER2-targeted treatment regimen for a minimum of 12 months. All participants will undergo echocardiograms before and 6-, 12-, and 18-months after initiation of HER2-targeted treatment. The primary composite outcome is symptomatic heart failure (New York Heart Association class III or IV) or death from cardiovascular causes. Secondary outcomes include: 1) echocardiographic indices of left ventricular systolic function; 2) incidence of cardiotoxicity, defined by a ≥ 10% absolute reduction in left ventricular ejection fraction (LVEF) from baseline to < 53%; and 3) incidence of early interruption of HER2-targeted therapy.</p><p><strong>Conclusions: </strong>To our knowledge, this will be the first prospective study of a risk-based approach to cardiotoxicity surveillance. We expect findings from this study will inform the development of updated clinical practice guidelines to improve cardiotoxicity surveillance practices during HER2-positive breast cancer treatment.</p><p><strong>Trial registration: </strong>The trial was registered in the ClinicalTrials.gov registry (identifier NCT03983382) on June 12, 2019.</p>","PeriodicalId":72525,"journal":{"name":"","volume":"9 1","pages":"13"},"PeriodicalIF":0.0,"publicationDate":"2023-03-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9996968/pdf/","citationCount":"2","resultStr":"{\"title\":\"Rationale and design of a cardiac safety study for reduced cardiotoxicity surveillance during HER2-targeted therapy.\",\"authors\":\"Anthony F Yu, Chau T Dang, Justine Jorgensen, Chaya S Moskowitz, Patricia DeFusco, Eric Oligino, Kevin C Oeffinger, Jennifer E Liu, Richard M Steingart\",\"doi\":\"10.1186/s40959-023-00163-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Echocardiograms are recommended every 3 months in patients receiving human epidermal growth factor 2 (HER2)-targeted therapy for surveillance of left ventricular ejection fraction (LVEF). Efforts to tailor treatment for HER2-positive breast cancer have led to greater use of non-anthracycline regimens that are associated with lower cardiotoxicity risk, raising into question the need for frequent cardiotoxicity surveillance for these patients. This study seeks to evaluate whether less frequent cardiotoxicity surveillance (every 6 months) is safe for patients receiving a non-anthracycline HER2-targeted treatment regimen.</p><p><strong>Methods/design: </strong>We will enroll 190 women with histologically confirmed HER2-positive breast cancer scheduled to receive a non-anthracycline HER2-targeted treatment regimen for a minimum of 12 months. All participants will undergo echocardiograms before and 6-, 12-, and 18-months after initiation of HER2-targeted treatment. The primary composite outcome is symptomatic heart failure (New York Heart Association class III or IV) or death from cardiovascular causes. Secondary outcomes include: 1) echocardiographic indices of left ventricular systolic function; 2) incidence of cardiotoxicity, defined by a ≥ 10% absolute reduction in left ventricular ejection fraction (LVEF) from baseline to < 53%; and 3) incidence of early interruption of HER2-targeted therapy.</p><p><strong>Conclusions: </strong>To our knowledge, this will be the first prospective study of a risk-based approach to cardiotoxicity surveillance. We expect findings from this study will inform the development of updated clinical practice guidelines to improve cardiotoxicity surveillance practices during HER2-positive breast cancer treatment.</p><p><strong>Trial registration: </strong>The trial was registered in the ClinicalTrials.gov registry (identifier NCT03983382) on June 12, 2019.</p>\",\"PeriodicalId\":72525,\"journal\":{\"name\":\"\",\"volume\":\"9 1\",\"pages\":\"13\"},\"PeriodicalIF\":0.0,\"publicationDate\":\"2023-03-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9996968/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40959-023-00163-4\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-023-00163-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Rationale and design of a cardiac safety study for reduced cardiotoxicity surveillance during HER2-targeted therapy.
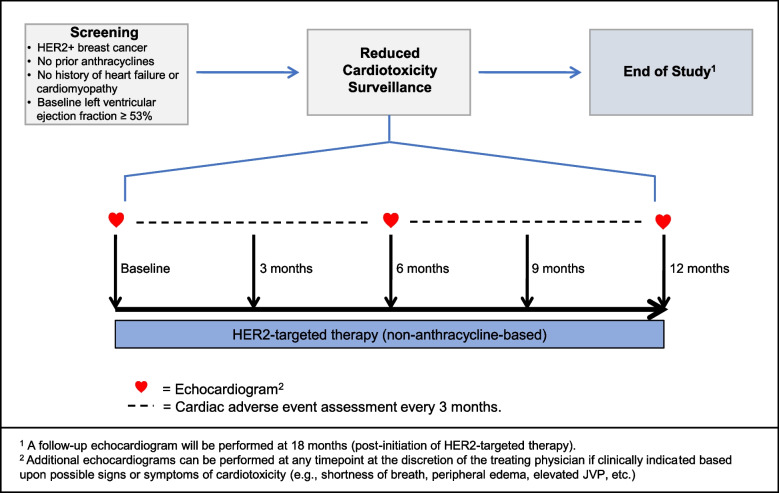
Background: Echocardiograms are recommended every 3 months in patients receiving human epidermal growth factor 2 (HER2)-targeted therapy for surveillance of left ventricular ejection fraction (LVEF). Efforts to tailor treatment for HER2-positive breast cancer have led to greater use of non-anthracycline regimens that are associated with lower cardiotoxicity risk, raising into question the need for frequent cardiotoxicity surveillance for these patients. This study seeks to evaluate whether less frequent cardiotoxicity surveillance (every 6 months) is safe for patients receiving a non-anthracycline HER2-targeted treatment regimen.
Methods/design: We will enroll 190 women with histologically confirmed HER2-positive breast cancer scheduled to receive a non-anthracycline HER2-targeted treatment regimen for a minimum of 12 months. All participants will undergo echocardiograms before and 6-, 12-, and 18-months after initiation of HER2-targeted treatment. The primary composite outcome is symptomatic heart failure (New York Heart Association class III or IV) or death from cardiovascular causes. Secondary outcomes include: 1) echocardiographic indices of left ventricular systolic function; 2) incidence of cardiotoxicity, defined by a ≥ 10% absolute reduction in left ventricular ejection fraction (LVEF) from baseline to < 53%; and 3) incidence of early interruption of HER2-targeted therapy.
Conclusions: To our knowledge, this will be the first prospective study of a risk-based approach to cardiotoxicity surveillance. We expect findings from this study will inform the development of updated clinical practice guidelines to improve cardiotoxicity surveillance practices during HER2-positive breast cancer treatment.
Trial registration: The trial was registered in the ClinicalTrials.gov registry (identifier NCT03983382) on June 12, 2019.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


