Taher Said Abd Elkareem, Taghreed Abdelrahman Ahmed, Layla Ahmed Mohamed
{"title":"二维和三维斑点跟踪超声心动图在严重风湿性二尖瓣狭窄和窦性心律患者左房重构中的应用。","authors":"Taher Said Abd Elkareem, Taghreed Abdelrahman Ahmed, Layla Ahmed Mohamed","doi":"10.14740/cr1465","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In mitral stenosis (MS), the combination of an increase in left atrium (LA) pressure and atrial inflammatory response is accompanied by increase in interstitial fibrosis of the atrial wall with disorganization of atrial muscle bundles, LA dysfunction and subsequently LA dilatation. We aimed to assess the effect of severe rheumatic MS on LA volumes and mechanics.</p><p><strong>Methods: </strong>We enrolled 40 patients with pure severe rheumatic MS and sinus rhythm as a patient group and 30 healthy subjects as a control group. All patient and control groups underwent two-dimensional (2D) transthoracic echo to measure left ventricle (LV) dimensions, function, LA deformations, estimated systolic pulmonary artery pressure (EPAP), and left ventricle global longitudinal strain (LV GLS). Also LA volumes and mechanics (LA strain during LV systole (reservoir function) and LV diastole (early = conduit, and late = booster pump = atrial contraction)) were measured by three-dimensional (3D) transthoracic echo; mitral valve (MV) area was measured by 3D transesophageal echo (as routine pre-percutaneous MV commissurotomy using multiplanar reconstruction in mid-esophageal apical long-axis view from LA prospective).</p><p><strong>Results: </strong>By 2D transthoracic echo, patient group revealed significantly lower all LA function vs. control group including LA strain during reservoir (24 ± 6 vs. 43 ± 3, P < 0.001), LA strain during conduit (-11 ± 3 vs. -25 ± 2, P < 0.001), and during booster pump (-13 ± 4 vs. -18 ± 1, P < 0.001). EPAP was significantly higher in patient group (48 ± 7 vs. 27 ± 4 in control group). LV GLS was significantly lower in patient group (-16±2% vs. -23±2% in control group). All 3D LA volumes were significantly higher in patient group than control group including maximum LA volume (LAVmax) (76 ± 18 vs. 50 ± 5, P < 0.001), indexed LA volume (LAVi) (44.6 ± 10.1 vs. 28.7 ± 3.7, P < 0.001), LV minimum volume (LAVmin) (51 ± 15 vs. 30 ± 4, P < 0.001), and LA volume pre atrial contraction (LAVpre A) (63 ± 15 vs. 41 ± 6, P < 0.001). Also, there was significantly decreased LA strain using 3D speckle tracking echo in patient group including systolic deformation of LA (reservoir function) (23 ± 6 vs. 41 ± 3, P < 0.001) and diastolic deformation, early diastole (conduit function) (-10 ± 2 vs. -24 ± 2, P < 0.001), and late diastole (booster pump function) (-13 ± 4 vs. -18 ± 1, P < 0.001).</p><p><strong>Conclusions: </strong>All LA function markedly reduced in pure severe rheumatic MS. The reduction of LA mechanics is directly related to the degree of reduction of the stenotic MV area. LV GLS significantly reduced in severe MS and its reduction is directly related to the degree of reduction of the stenotic MV area and the LAVi by 3D echo.</p>","PeriodicalId":9424,"journal":{"name":"Cardiology Research","volume":"14 2","pages":"142-148"},"PeriodicalIF":1.4000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a5/0e/cr-14-142.PMC10116933.pdf","citationCount":"0","resultStr":"{\"title\":\"Left Atrial Remodeling in Patients With Severe Rheumatic Mitral Stenosis and Sinus Rhythm Using Two-Dimensional and Three-Dimensional Speckle Tracking Echocardiography.\",\"authors\":\"Taher Said Abd Elkareem, Taghreed Abdelrahman Ahmed, Layla Ahmed Mohamed\",\"doi\":\"10.14740/cr1465\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>In mitral stenosis (MS), the combination of an increase in left atrium (LA) pressure and atrial inflammatory response is accompanied by increase in interstitial fibrosis of the atrial wall with disorganization of atrial muscle bundles, LA dysfunction and subsequently LA dilatation. We aimed to assess the effect of severe rheumatic MS on LA volumes and mechanics.</p><p><strong>Methods: </strong>We enrolled 40 patients with pure severe rheumatic MS and sinus rhythm as a patient group and 30 healthy subjects as a control group. All patient and control groups underwent two-dimensional (2D) transthoracic echo to measure left ventricle (LV) dimensions, function, LA deformations, estimated systolic pulmonary artery pressure (EPAP), and left ventricle global longitudinal strain (LV GLS). Also LA volumes and mechanics (LA strain during LV systole (reservoir function) and LV diastole (early = conduit, and late = booster pump = atrial contraction)) were measured by three-dimensional (3D) transthoracic echo; mitral valve (MV) area was measured by 3D transesophageal echo (as routine pre-percutaneous MV commissurotomy using multiplanar reconstruction in mid-esophageal apical long-axis view from LA prospective).</p><p><strong>Results: </strong>By 2D transthoracic echo, patient group revealed significantly lower all LA function vs. control group including LA strain during reservoir (24 ± 6 vs. 43 ± 3, P < 0.001), LA strain during conduit (-11 ± 3 vs. -25 ± 2, P < 0.001), and during booster pump (-13 ± 4 vs. -18 ± 1, P < 0.001). EPAP was significantly higher in patient group (48 ± 7 vs. 27 ± 4 in control group). LV GLS was significantly lower in patient group (-16±2% vs. -23±2% in control group). All 3D LA volumes were significantly higher in patient group than control group including maximum LA volume (LAVmax) (76 ± 18 vs. 50 ± 5, P < 0.001), indexed LA volume (LAVi) (44.6 ± 10.1 vs. 28.7 ± 3.7, P < 0.001), LV minimum volume (LAVmin) (51 ± 15 vs. 30 ± 4, P < 0.001), and LA volume pre atrial contraction (LAVpre A) (63 ± 15 vs. 41 ± 6, P < 0.001). Also, there was significantly decreased LA strain using 3D speckle tracking echo in patient group including systolic deformation of LA (reservoir function) (23 ± 6 vs. 41 ± 3, P < 0.001) and diastolic deformation, early diastole (conduit function) (-10 ± 2 vs. -24 ± 2, P < 0.001), and late diastole (booster pump function) (-13 ± 4 vs. -18 ± 1, P < 0.001).</p><p><strong>Conclusions: </strong>All LA function markedly reduced in pure severe rheumatic MS. The reduction of LA mechanics is directly related to the degree of reduction of the stenotic MV area. LV GLS significantly reduced in severe MS and its reduction is directly related to the degree of reduction of the stenotic MV area and the LAVi by 3D echo.</p>\",\"PeriodicalId\":9424,\"journal\":{\"name\":\"Cardiology Research\",\"volume\":\"14 2\",\"pages\":\"142-148\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2023-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a5/0e/cr-14-142.PMC10116933.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiology Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/cr1465\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/cr1465","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Left Atrial Remodeling in Patients With Severe Rheumatic Mitral Stenosis and Sinus Rhythm Using Two-Dimensional and Three-Dimensional Speckle Tracking Echocardiography.
Background: In mitral stenosis (MS), the combination of an increase in left atrium (LA) pressure and atrial inflammatory response is accompanied by increase in interstitial fibrosis of the atrial wall with disorganization of atrial muscle bundles, LA dysfunction and subsequently LA dilatation. We aimed to assess the effect of severe rheumatic MS on LA volumes and mechanics.
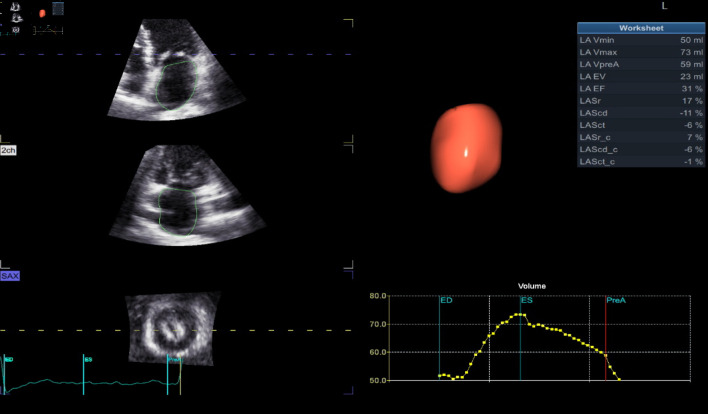
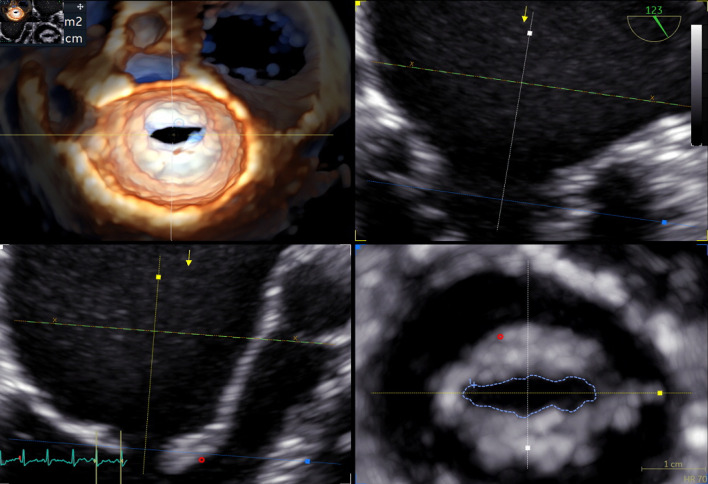
Methods: We enrolled 40 patients with pure severe rheumatic MS and sinus rhythm as a patient group and 30 healthy subjects as a control group. All patient and control groups underwent two-dimensional (2D) transthoracic echo to measure left ventricle (LV) dimensions, function, LA deformations, estimated systolic pulmonary artery pressure (EPAP), and left ventricle global longitudinal strain (LV GLS). Also LA volumes and mechanics (LA strain during LV systole (reservoir function) and LV diastole (early = conduit, and late = booster pump = atrial contraction)) were measured by three-dimensional (3D) transthoracic echo; mitral valve (MV) area was measured by 3D transesophageal echo (as routine pre-percutaneous MV commissurotomy using multiplanar reconstruction in mid-esophageal apical long-axis view from LA prospective).
Results: By 2D transthoracic echo, patient group revealed significantly lower all LA function vs. control group including LA strain during reservoir (24 ± 6 vs. 43 ± 3, P < 0.001), LA strain during conduit (-11 ± 3 vs. -25 ± 2, P < 0.001), and during booster pump (-13 ± 4 vs. -18 ± 1, P < 0.001). EPAP was significantly higher in patient group (48 ± 7 vs. 27 ± 4 in control group). LV GLS was significantly lower in patient group (-16±2% vs. -23±2% in control group). All 3D LA volumes were significantly higher in patient group than control group including maximum LA volume (LAVmax) (76 ± 18 vs. 50 ± 5, P < 0.001), indexed LA volume (LAVi) (44.6 ± 10.1 vs. 28.7 ± 3.7, P < 0.001), LV minimum volume (LAVmin) (51 ± 15 vs. 30 ± 4, P < 0.001), and LA volume pre atrial contraction (LAVpre A) (63 ± 15 vs. 41 ± 6, P < 0.001). Also, there was significantly decreased LA strain using 3D speckle tracking echo in patient group including systolic deformation of LA (reservoir function) (23 ± 6 vs. 41 ± 3, P < 0.001) and diastolic deformation, early diastole (conduit function) (-10 ± 2 vs. -24 ± 2, P < 0.001), and late diastole (booster pump function) (-13 ± 4 vs. -18 ± 1, P < 0.001).
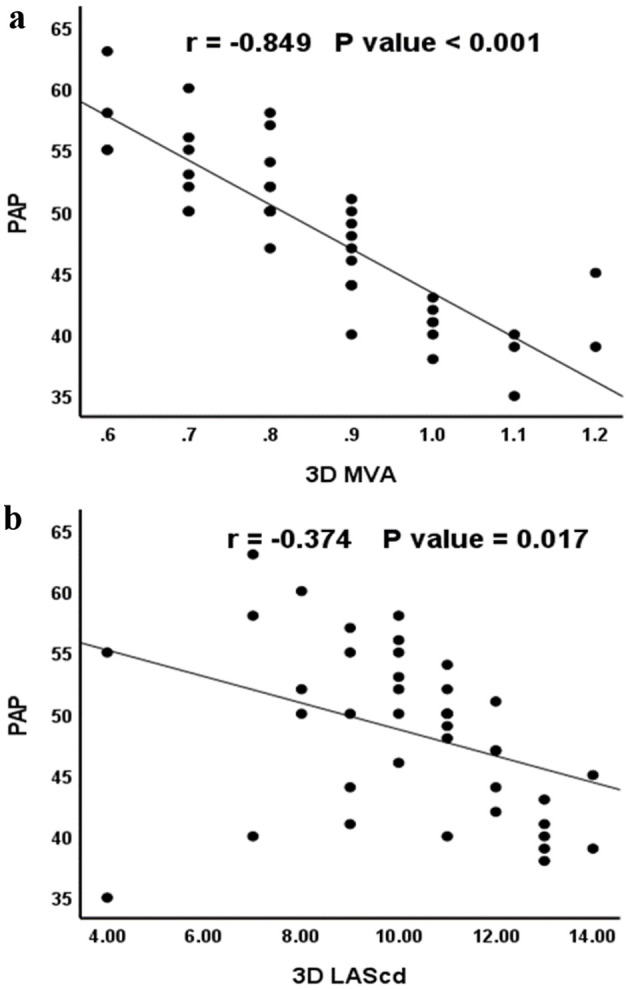
Conclusions: All LA function markedly reduced in pure severe rheumatic MS. The reduction of LA mechanics is directly related to the degree of reduction of the stenotic MV area. LV GLS significantly reduced in severe MS and its reduction is directly related to the degree of reduction of the stenotic MV area and the LAVi by 3D echo.
期刊介绍:
Cardiology Research is an open access, peer-reviewed, international journal. All submissions relating to basic research and clinical practice of cardiology and cardiovascular medicine are in this journal''s scope. This journal focuses on publishing original research and observations in all cardiovascular medicine aspects. Manuscript types include original article, review, case report, short communication, book review, letter to the editor.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


