{"title":"南非约翰内斯堡一家学术医院三级儿科重症监护病房的高频振荡通气。","authors":"S Cawood, B Rae, K D Naidoo","doi":"10.7196/SAJCC.2019.v35i2.396","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>High-frequency oscillatory ventilation (HFOV) remains an option for the management of critically ill children when conventional mechanical ventilation fails. However, its use is not widespread, and there is wide variability reported with respect to how it is used.</p><p><strong>Objectives: </strong>To describe the frequency, indications, settings and outcomes of HFOV use among paediatric patients with a primary respiratory disorder admitted to a tertiary paediatric intensive care unit (PICU).</p><p><strong>Methods: </strong>The study was a 2-year, single-centre, retrospective chart review.</p><p><strong>Results: </strong>Thirty-four (32.7%) patients were managed with HFOV in the PICU during the study period. Thirty-three of the 34 patients had paediatric acute respiratory distress syndrome. Indications for HFOV were inadequate oxygenation in 17 patients (50%), and refractory respiratory acidosis in 15 patients (44.1%) (2 patients did not fit into either category). Approaches to the setting of HFOV varied considerably, particularly with respect to initial pressure around the airways. HFOV was effective at improving both oxygenation, with a median (interquartile range (IQR)) decrease in oxygenation index of 6.34 (5.0 - 9.5), and ventilation with a the median decrease in PaCO<sub>2</sub> of 67.6 (46.2 - 105.7) mmHg after 24 hours. Overall mortality was 29.4% in the HFOV group, which is consistent with other studies.</p><p><strong>Conclusion: </strong>HFOV remains an effective rescue ventilatory strategy, which resulted in rapid and sustained improvement in gas exchange in patients with severe hypoxaemia and/or severe respiratory acidosis, particularly in the absence of extracorporeal support. However, the variability in practice and the adverse effects described highlight the need for future high-quality randomised controlled trials to allow for development of meaningful guidelines to optimise HFOV use.</p><p><strong>Contributions of the study: </strong>This study describes the use and outcomes of high-frequency oscillatory ventilation (HFOV) in a South African paediatric intensive care unit, thus addressing a local knowledge gap and providing evidence of the continued efficacy of HFOV for severe hypoxaemia and refractory respiratory acidosis in settings without access to extracorporeal technologies.</p>","PeriodicalId":75194,"journal":{"name":"The Southern African journal of critical care : the official journal of the Critical Care Society","volume":"35 2","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2019-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.7196/SAJCC.2019.v35i2.396","citationCount":"1","resultStr":"{\"title\":\"High-frequency oscillatory ventilation in a tertiary paediatric intensive care unit in an academic hospital in Johannesburg, South Africa.\",\"authors\":\"S Cawood, B Rae, K D Naidoo\",\"doi\":\"10.7196/SAJCC.2019.v35i2.396\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>High-frequency oscillatory ventilation (HFOV) remains an option for the management of critically ill children when conventional mechanical ventilation fails. However, its use is not widespread, and there is wide variability reported with respect to how it is used.</p><p><strong>Objectives: </strong>To describe the frequency, indications, settings and outcomes of HFOV use among paediatric patients with a primary respiratory disorder admitted to a tertiary paediatric intensive care unit (PICU).</p><p><strong>Methods: </strong>The study was a 2-year, single-centre, retrospective chart review.</p><p><strong>Results: </strong>Thirty-four (32.7%) patients were managed with HFOV in the PICU during the study period. Thirty-three of the 34 patients had paediatric acute respiratory distress syndrome. Indications for HFOV were inadequate oxygenation in 17 patients (50%), and refractory respiratory acidosis in 15 patients (44.1%) (2 patients did not fit into either category). Approaches to the setting of HFOV varied considerably, particularly with respect to initial pressure around the airways. HFOV was effective at improving both oxygenation, with a median (interquartile range (IQR)) decrease in oxygenation index of 6.34 (5.0 - 9.5), and ventilation with a the median decrease in PaCO<sub>2</sub> of 67.6 (46.2 - 105.7) mmHg after 24 hours. Overall mortality was 29.4% in the HFOV group, which is consistent with other studies.</p><p><strong>Conclusion: </strong>HFOV remains an effective rescue ventilatory strategy, which resulted in rapid and sustained improvement in gas exchange in patients with severe hypoxaemia and/or severe respiratory acidosis, particularly in the absence of extracorporeal support. However, the variability in practice and the adverse effects described highlight the need for future high-quality randomised controlled trials to allow for development of meaningful guidelines to optimise HFOV use.</p><p><strong>Contributions of the study: </strong>This study describes the use and outcomes of high-frequency oscillatory ventilation (HFOV) in a South African paediatric intensive care unit, thus addressing a local knowledge gap and providing evidence of the continued efficacy of HFOV for severe hypoxaemia and refractory respiratory acidosis in settings without access to extracorporeal technologies.</p>\",\"PeriodicalId\":75194,\"journal\":{\"name\":\"The Southern African journal of critical care : the official journal of the Critical Care Society\",\"volume\":\"35 2\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2019-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.7196/SAJCC.2019.v35i2.396\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Southern African journal of critical care : the official journal of the Critical Care Society\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.7196/SAJCC.2019.v35i2.396\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Southern African journal of critical care : the official journal of the Critical Care Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7196/SAJCC.2019.v35i2.396","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
High-frequency oscillatory ventilation in a tertiary paediatric intensive care unit in an academic hospital in Johannesburg, South Africa.
Background: High-frequency oscillatory ventilation (HFOV) remains an option for the management of critically ill children when conventional mechanical ventilation fails. However, its use is not widespread, and there is wide variability reported with respect to how it is used.
Objectives: To describe the frequency, indications, settings and outcomes of HFOV use among paediatric patients with a primary respiratory disorder admitted to a tertiary paediatric intensive care unit (PICU).
Methods: The study was a 2-year, single-centre, retrospective chart review.
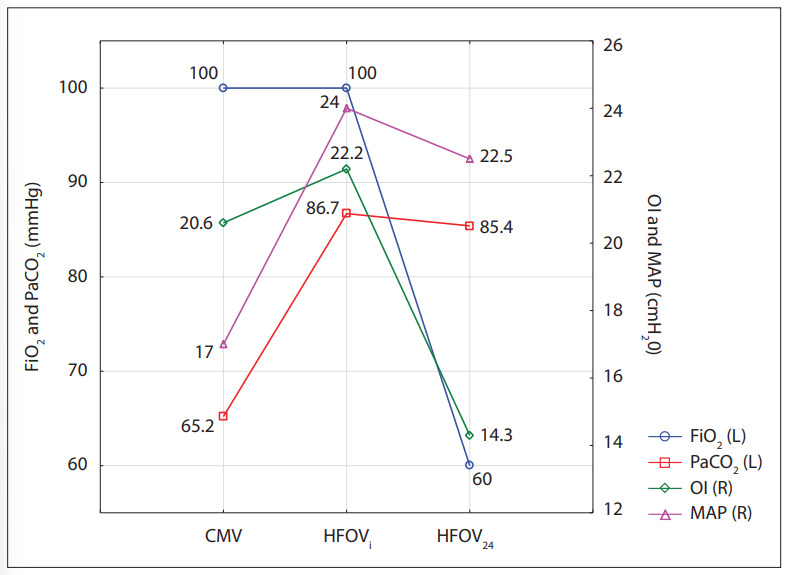
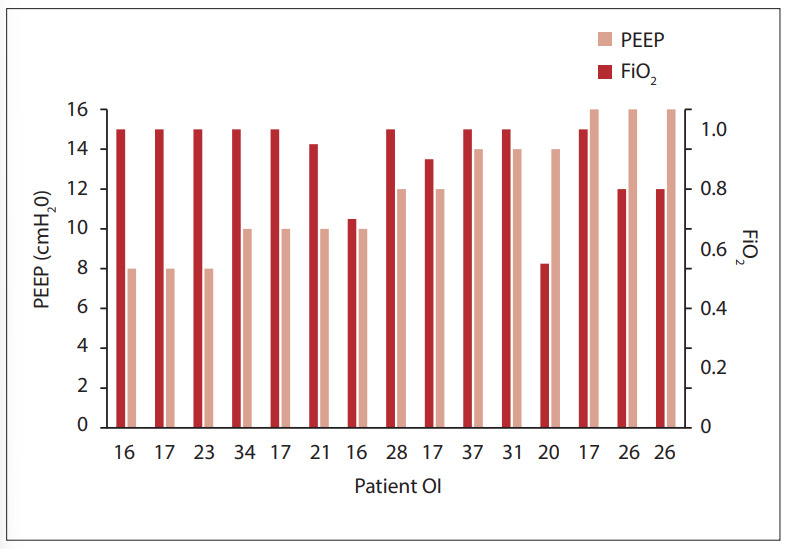
Results: Thirty-four (32.7%) patients were managed with HFOV in the PICU during the study period. Thirty-three of the 34 patients had paediatric acute respiratory distress syndrome. Indications for HFOV were inadequate oxygenation in 17 patients (50%), and refractory respiratory acidosis in 15 patients (44.1%) (2 patients did not fit into either category). Approaches to the setting of HFOV varied considerably, particularly with respect to initial pressure around the airways. HFOV was effective at improving both oxygenation, with a median (interquartile range (IQR)) decrease in oxygenation index of 6.34 (5.0 - 9.5), and ventilation with a the median decrease in PaCO2 of 67.6 (46.2 - 105.7) mmHg after 24 hours. Overall mortality was 29.4% in the HFOV group, which is consistent with other studies.
Conclusion: HFOV remains an effective rescue ventilatory strategy, which resulted in rapid and sustained improvement in gas exchange in patients with severe hypoxaemia and/or severe respiratory acidosis, particularly in the absence of extracorporeal support. However, the variability in practice and the adverse effects described highlight the need for future high-quality randomised controlled trials to allow for development of meaningful guidelines to optimise HFOV use.
Contributions of the study: This study describes the use and outcomes of high-frequency oscillatory ventilation (HFOV) in a South African paediatric intensive care unit, thus addressing a local knowledge gap and providing evidence of the continued efficacy of HFOV for severe hypoxaemia and refractory respiratory acidosis in settings without access to extracorporeal technologies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


