Jesse M Hinde, Bryan R Garner, Colleen J Watson, Rasika Ramanan, Elizabeth L Ball, Stephen J Tueller
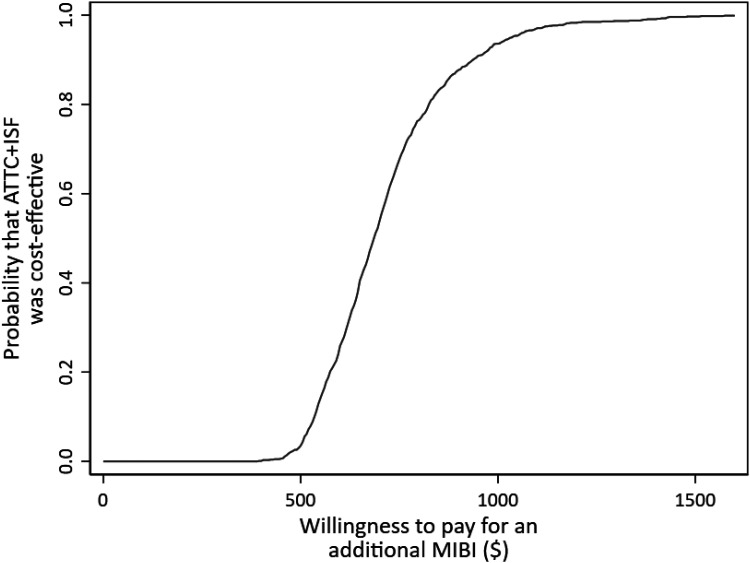
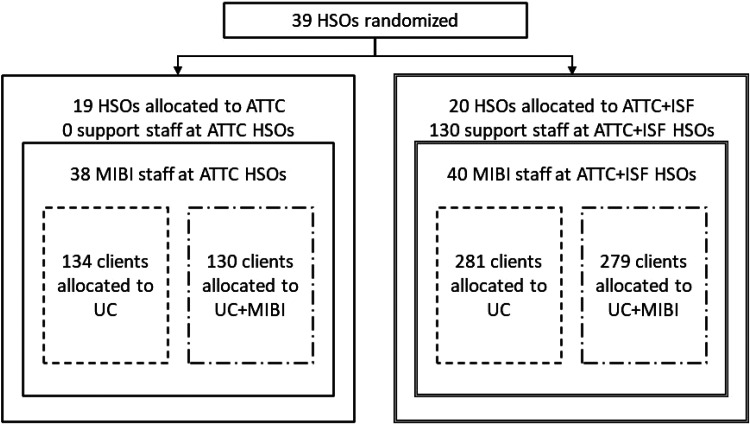
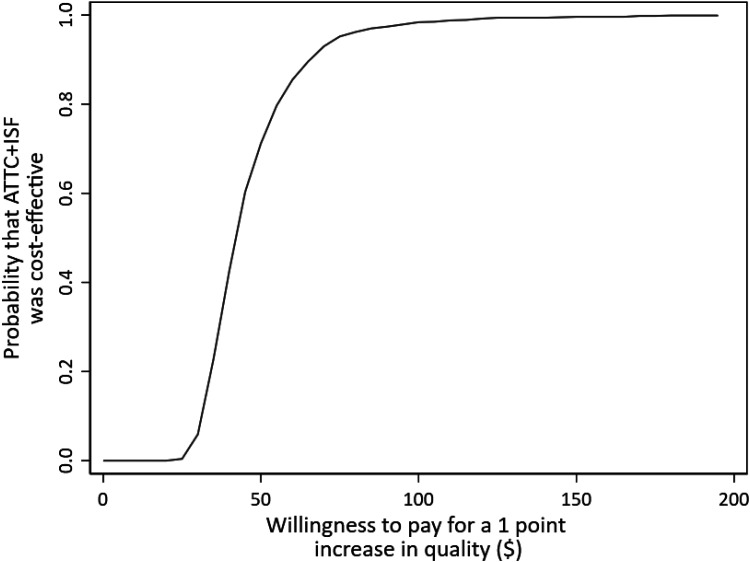
{"title":"实施和维持促进(ISF)战略:39个站点的集群随机试验的成本和成本效益结果,该试验整合了社区艾滋病毒服务组织的药物使用服务。","authors":"Jesse M Hinde, Bryan R Garner, Colleen J Watson, Rasika Ramanan, Elizabeth L Ball, Stephen J Tueller","doi":"10.1177/26334895221089266","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> As part of the Substance Abuse Treatment to HIV Care Project, the Implementation & Sustainment Facilitation (ISF) strategy was found to be an effective adjunct to the Addiction Technology Transfer Center (ATTC) strategy for integrating a motivational interviewing-based brief intervention (MIBI) for substance use disorders. This study presents the cost and cost-effectiveness results. <b>Methods:</b> Thirty-nine HIV service organizations were randomized to receive the ATTC-only condition or the ATTC + ISF condition. Two staff from each organization received the ATTC-training. In ATTC + ISF organizations, the same two staff and additional support staff participated in facilitation sessions to support MIBI implementation. We estimated costs using primary data on the time spent in each strategy and the time spent delivering 409 MIBIs to clients. We estimated staff-level cost-effectiveness for the number of MIBIs delivered, average MIBI quality scores, and total client days abstinent per staff. We used sensitivity analyses to test how changes to key variables affect the results. <b>Results:</b> Adjusted per-staff costs were $2,915 for the ATTC strategy and $5,371 for ATTC + ISF, resulting in an incremental cost of $2,457. ATTC + ISF significantly increased the number of MIBIs delivered (3.73) and the average MIBI quality score (61.45), yielding incremental cost effectiveness ratios (ICERs) of $659 and $40. Client days abstinent increased by 59 days per staff with a quality-adjusted life-year ICER of $40,578 (95% confidence interval $29,795-$61,031). <b>Conclusions:</b> From the perspective of federal policymakers, ISF as an adjunct to the ATTC strategy may be cost-effective for improving the integration of MIBIs within HIV service organizations, especially if scaled up to reach more clients. Travel accounted for nearly half of costs, and virtual implementation may further increase value. We also highlight two considerations for cost-effectiveness analysis with hybrid trials: study protocols kept recruitment low and modeling choices affect how we interpret the effects on client-level outcomes.</p>","PeriodicalId":73354,"journal":{"name":"Implementation research and practice","volume":"3 ","pages":"26334895221089266"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/2b/38/10.1177_26334895221089266.PMC9924275.pdf","citationCount":"2","resultStr":"{\"title\":\"The implementation & sustainment facilitation (ISF) strategy: Cost and cost-effectiveness results from a 39-site cluster randomized trial integrating substance use services in community-based HIV service organizations.\",\"authors\":\"Jesse M Hinde, Bryan R Garner, Colleen J Watson, Rasika Ramanan, Elizabeth L Ball, Stephen J Tueller\",\"doi\":\"10.1177/26334895221089266\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> As part of the Substance Abuse Treatment to HIV Care Project, the Implementation & Sustainment Facilitation (ISF) strategy was found to be an effective adjunct to the Addiction Technology Transfer Center (ATTC) strategy for integrating a motivational interviewing-based brief intervention (MIBI) for substance use disorders. This study presents the cost and cost-effectiveness results. <b>Methods:</b> Thirty-nine HIV service organizations were randomized to receive the ATTC-only condition or the ATTC + ISF condition. Two staff from each organization received the ATTC-training. In ATTC + ISF organizations, the same two staff and additional support staff participated in facilitation sessions to support MIBI implementation. We estimated costs using primary data on the time spent in each strategy and the time spent delivering 409 MIBIs to clients. We estimated staff-level cost-effectiveness for the number of MIBIs delivered, average MIBI quality scores, and total client days abstinent per staff. We used sensitivity analyses to test how changes to key variables affect the results. <b>Results:</b> Adjusted per-staff costs were $2,915 for the ATTC strategy and $5,371 for ATTC + ISF, resulting in an incremental cost of $2,457. ATTC + ISF significantly increased the number of MIBIs delivered (3.73) and the average MIBI quality score (61.45), yielding incremental cost effectiveness ratios (ICERs) of $659 and $40. Client days abstinent increased by 59 days per staff with a quality-adjusted life-year ICER of $40,578 (95% confidence interval $29,795-$61,031). <b>Conclusions:</b> From the perspective of federal policymakers, ISF as an adjunct to the ATTC strategy may be cost-effective for improving the integration of MIBIs within HIV service organizations, especially if scaled up to reach more clients. Travel accounted for nearly half of costs, and virtual implementation may further increase value. We also highlight two considerations for cost-effectiveness analysis with hybrid trials: study protocols kept recruitment low and modeling choices affect how we interpret the effects on client-level outcomes.</p>\",\"PeriodicalId\":73354,\"journal\":{\"name\":\"Implementation research and practice\",\"volume\":\"3 \",\"pages\":\"26334895221089266\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/2b/38/10.1177_26334895221089266.PMC9924275.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Implementation research and practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/26334895221089266\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26334895221089266","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
The implementation & sustainment facilitation (ISF) strategy: Cost and cost-effectiveness results from a 39-site cluster randomized trial integrating substance use services in community-based HIV service organizations.
Background: As part of the Substance Abuse Treatment to HIV Care Project, the Implementation & Sustainment Facilitation (ISF) strategy was found to be an effective adjunct to the Addiction Technology Transfer Center (ATTC) strategy for integrating a motivational interviewing-based brief intervention (MIBI) for substance use disorders. This study presents the cost and cost-effectiveness results. Methods: Thirty-nine HIV service organizations were randomized to receive the ATTC-only condition or the ATTC + ISF condition. Two staff from each organization received the ATTC-training. In ATTC + ISF organizations, the same two staff and additional support staff participated in facilitation sessions to support MIBI implementation. We estimated costs using primary data on the time spent in each strategy and the time spent delivering 409 MIBIs to clients. We estimated staff-level cost-effectiveness for the number of MIBIs delivered, average MIBI quality scores, and total client days abstinent per staff. We used sensitivity analyses to test how changes to key variables affect the results. Results: Adjusted per-staff costs were $2,915 for the ATTC strategy and $5,371 for ATTC + ISF, resulting in an incremental cost of $2,457. ATTC + ISF significantly increased the number of MIBIs delivered (3.73) and the average MIBI quality score (61.45), yielding incremental cost effectiveness ratios (ICERs) of $659 and $40. Client days abstinent increased by 59 days per staff with a quality-adjusted life-year ICER of $40,578 (95% confidence interval $29,795-$61,031). Conclusions: From the perspective of federal policymakers, ISF as an adjunct to the ATTC strategy may be cost-effective for improving the integration of MIBIs within HIV service organizations, especially if scaled up to reach more clients. Travel accounted for nearly half of costs, and virtual implementation may further increase value. We also highlight two considerations for cost-effectiveness analysis with hybrid trials: study protocols kept recruitment low and modeling choices affect how we interpret the effects on client-level outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


