S M Savarimuthu, C Cairns, N L Allorto, G E Weissman, R Kohn, R D Wise, G L Anesi
{"title":"qSOFA作为南非夸祖鲁-纳塔尔省资源有限环境下ICU预后的预测因子","authors":"S M Savarimuthu, C Cairns, N L Allorto, G E Weissman, R Kohn, R D Wise, G L Anesi","doi":"10.7196/SAJCC.2020.v36i2.433","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Sepsis is a major cause of morbidity and mortality, especially in critical care patients. Developing tools to identify patients who are at risk of poor outcomes and prolonged length of stay in intensive care units (ICUs) is critical, particularly in resource-limited settings.</p><p><strong>Objectives: </strong>To determine whether the quick sequential organ failure assessment (qSOFA) score based on bedside assessment alone was a promising tool for risk prediction in low-resource settings.</p><p><strong>Methods: </strong>A retrospective cohort of adult patients admitted to the intensive care unit (ICU) at Edendale Hospital in Pietermaritzburg, South Africa (SA), was recruited into the study between 2014 and 2018. The association of qSOFA with in-ICU mortality was measured using multivariable logistic regression. Discrimination was assessed using the area under the receiver operating characteristic curve and the additive contribution to a baseline model using likelihood ratio testing.</p><p><strong>Results: </strong>The qSOFA scores of 0, 1 and 2 were not associated with increased odds of in-ICU mortality (adjusted odds ratio (aOR) 1.24, 95% confidence interval (CI) 0.86 - 1.79; <i>p</i>=0.26) in patients with infection, while the qSOFA of 3 was associated with in-ICU mortality in infected patients (aOR 2.82; 95% CI 1.91 - 4.16; <i>p</i><0.001). On the other hand, the qSOFA scores of 2 (aOR 3.25; 95% CI 1.91 - 5.53; <i>p</i><0.001) and 3 (aOR 6.26, 95% CI 0.38 - 11.62, <i>p</i><0.001) were associated with increased odds of in-ICU mortality in patients without infection. Discrimination for mortality was fair to poor and adding qSOFA to a baseline model yielded a statistical improvement in both cases (<i>p</i><0.001).</p><p><strong>Conclusion: </strong>qSOFA was associated with, but weakly discriminant, for in-ICU mortality for patients with and without infection in a resource-limited, public hospital in SA. These findings add to the growing body of evidence that support the use of qSOFA to deliver low-cost, high-value critical care in resource-limited settings.</p><p><strong>Contributions of the study: </strong>This study expanded the data supporting the use of qSOFA in resource-limited settings beyond the emergency department or ward to include patients admitted to the ICU. Additionally, this study demonstrated stronger predictive abilities in a population of patients admitted with trauma without suspected or confirmed infection, thus providing an additional use of qSOFA as a risk-prediction tool for a broader population.</p>","PeriodicalId":75194,"journal":{"name":"The Southern African journal of critical care : the official journal of the Critical Care Society","volume":"36 2","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2020-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/bf/9f/SAJCC-36-2-433.PMC9045512.pdf","citationCount":"5","resultStr":"{\"title\":\"qSOFA as a predictor of ICU outcomes in a resource-limited setting in KwaZulu-Natal Province, South Africa.\",\"authors\":\"S M Savarimuthu, C Cairns, N L Allorto, G E Weissman, R Kohn, R D Wise, G L Anesi\",\"doi\":\"10.7196/SAJCC.2020.v36i2.433\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Sepsis is a major cause of morbidity and mortality, especially in critical care patients. Developing tools to identify patients who are at risk of poor outcomes and prolonged length of stay in intensive care units (ICUs) is critical, particularly in resource-limited settings.</p><p><strong>Objectives: </strong>To determine whether the quick sequential organ failure assessment (qSOFA) score based on bedside assessment alone was a promising tool for risk prediction in low-resource settings.</p><p><strong>Methods: </strong>A retrospective cohort of adult patients admitted to the intensive care unit (ICU) at Edendale Hospital in Pietermaritzburg, South Africa (SA), was recruited into the study between 2014 and 2018. The association of qSOFA with in-ICU mortality was measured using multivariable logistic regression. Discrimination was assessed using the area under the receiver operating characteristic curve and the additive contribution to a baseline model using likelihood ratio testing.</p><p><strong>Results: </strong>The qSOFA scores of 0, 1 and 2 were not associated with increased odds of in-ICU mortality (adjusted odds ratio (aOR) 1.24, 95% confidence interval (CI) 0.86 - 1.79; <i>p</i>=0.26) in patients with infection, while the qSOFA of 3 was associated with in-ICU mortality in infected patients (aOR 2.82; 95% CI 1.91 - 4.16; <i>p</i><0.001). On the other hand, the qSOFA scores of 2 (aOR 3.25; 95% CI 1.91 - 5.53; <i>p</i><0.001) and 3 (aOR 6.26, 95% CI 0.38 - 11.62, <i>p</i><0.001) were associated with increased odds of in-ICU mortality in patients without infection. Discrimination for mortality was fair to poor and adding qSOFA to a baseline model yielded a statistical improvement in both cases (<i>p</i><0.001).</p><p><strong>Conclusion: </strong>qSOFA was associated with, but weakly discriminant, for in-ICU mortality for patients with and without infection in a resource-limited, public hospital in SA. These findings add to the growing body of evidence that support the use of qSOFA to deliver low-cost, high-value critical care in resource-limited settings.</p><p><strong>Contributions of the study: </strong>This study expanded the data supporting the use of qSOFA in resource-limited settings beyond the emergency department or ward to include patients admitted to the ICU. Additionally, this study demonstrated stronger predictive abilities in a population of patients admitted with trauma without suspected or confirmed infection, thus providing an additional use of qSOFA as a risk-prediction tool for a broader population.</p>\",\"PeriodicalId\":75194,\"journal\":{\"name\":\"The Southern African journal of critical care : the official journal of the Critical Care Society\",\"volume\":\"36 2\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/bf/9f/SAJCC-36-2-433.PMC9045512.pdf\",\"citationCount\":\"5\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Southern African journal of critical care : the official journal of the Critical Care Society\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.7196/SAJCC.2020.v36i2.433\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Southern African journal of critical care : the official journal of the Critical Care Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7196/SAJCC.2020.v36i2.433","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 5
摘要
背景:脓毒症是发病率和死亡率的主要原因,特别是在重症监护患者中。开发工具来识别有预后不良风险和重症监护病房(icu)住院时间延长的患者至关重要,特别是在资源有限的环境中。目的:确定仅基于床边评估的快速顺序器官衰竭评估(qSOFA)评分是否为低资源环境下风险预测的一种有前景的工具。方法:回顾性研究纳入2014年至2018年在南非彼得马里茨堡Edendale医院重症监护室(ICU)住院的成年患者。采用多变量logistic回归分析qSOFA与icu死亡率的关系。使用受试者工作特征曲线下的面积和使用似然比检验对基线模型的附加贡献来评估歧视。结果:qSOFA评分0、1和2与icu内死亡率增加的几率无关(调整优势比(aOR) 1.24, 95%可信区间(CI) 0.86 - 1.79;p=0.26),而qSOFA为3与感染患者icu内死亡率相关(aOR为2.82;95% ci 1.91 - 4.16;结论:在SA资源有限的公立医院中,qSOFA与有感染和无感染患者的icu死亡率相关,但具有弱判别性。这些发现增加了越来越多的证据,支持在资源有限的环境中使用qSOFA提供低成本、高价值的重症监护。本研究的贡献:本研究扩大了支持qSOFA在资源有限的环境中使用的数据,超出了急诊科或病房,纳入了ICU住院的患者。此外,该研究表明,在没有疑似或确诊感染的创伤入院患者群体中,qSOFA具有更强的预测能力,从而为更广泛的人群提供了qSOFA作为风险预测工具的额外用途。
qSOFA as a predictor of ICU outcomes in a resource-limited setting in KwaZulu-Natal Province, South Africa.
Background: Sepsis is a major cause of morbidity and mortality, especially in critical care patients. Developing tools to identify patients who are at risk of poor outcomes and prolonged length of stay in intensive care units (ICUs) is critical, particularly in resource-limited settings.
Objectives: To determine whether the quick sequential organ failure assessment (qSOFA) score based on bedside assessment alone was a promising tool for risk prediction in low-resource settings.
Methods: A retrospective cohort of adult patients admitted to the intensive care unit (ICU) at Edendale Hospital in Pietermaritzburg, South Africa (SA), was recruited into the study between 2014 and 2018. The association of qSOFA with in-ICU mortality was measured using multivariable logistic regression. Discrimination was assessed using the area under the receiver operating characteristic curve and the additive contribution to a baseline model using likelihood ratio testing.
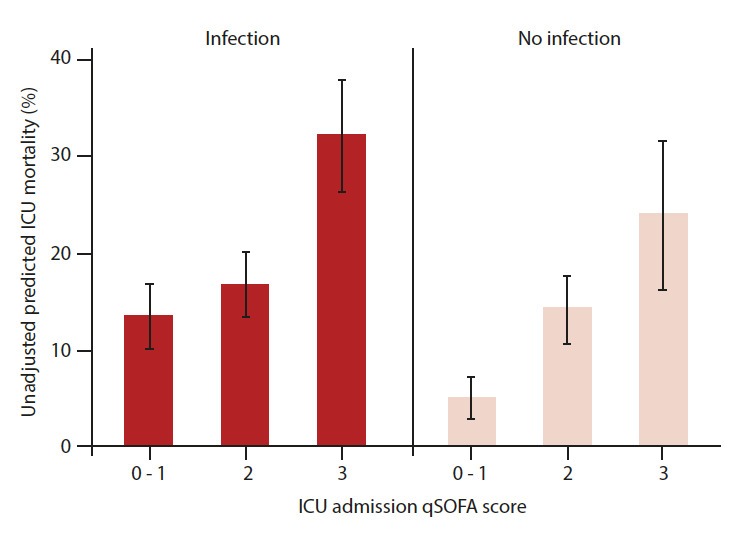
Results: The qSOFA scores of 0, 1 and 2 were not associated with increased odds of in-ICU mortality (adjusted odds ratio (aOR) 1.24, 95% confidence interval (CI) 0.86 - 1.79; p=0.26) in patients with infection, while the qSOFA of 3 was associated with in-ICU mortality in infected patients (aOR 2.82; 95% CI 1.91 - 4.16; p<0.001). On the other hand, the qSOFA scores of 2 (aOR 3.25; 95% CI 1.91 - 5.53; p<0.001) and 3 (aOR 6.26, 95% CI 0.38 - 11.62, p<0.001) were associated with increased odds of in-ICU mortality in patients without infection. Discrimination for mortality was fair to poor and adding qSOFA to a baseline model yielded a statistical improvement in both cases (p<0.001).
Conclusion: qSOFA was associated with, but weakly discriminant, for in-ICU mortality for patients with and without infection in a resource-limited, public hospital in SA. These findings add to the growing body of evidence that support the use of qSOFA to deliver low-cost, high-value critical care in resource-limited settings.
Contributions of the study: This study expanded the data supporting the use of qSOFA in resource-limited settings beyond the emergency department or ward to include patients admitted to the ICU. Additionally, this study demonstrated stronger predictive abilities in a population of patients admitted with trauma without suspected or confirmed infection, thus providing an additional use of qSOFA as a risk-prediction tool for a broader population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


