Prakirthi Yerram, Samantha N Reiss, Lisa Modelevsky, Lauren Schaff, Anne S Reiner, Katherine S Panageas, Christian Grommes
{"title":"越多越好吗?在一个大型原发性中枢神经系统淋巴瘤队列中,增加高剂量甲氨蝶呤和利妥昔单抗的剂量与改善预后相关。","authors":"Prakirthi Yerram, Samantha N Reiss, Lisa Modelevsky, Lauren Schaff, Anne S Reiner, Katherine S Panageas, Christian Grommes","doi":"10.21037/aol-22-19","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Primary central nervous system lymphoma (PCNSL) is a rare and aggressive primary brain tumor. While high dose methotrexate (HDMTX) regimens remain standard of care, it remains unclear if optimization of HDMTX doses and the addition of rituximab provide clinical benefit. Over the last 30 years, standard care given at Memorial Sloan Kettering Cancer Center (MSKCC) has evolved, allowing the comparison of patients receiving different numbers of HDMTX doses and those treated with and without rituximab. The purpose of this study was to describe outcomes based on treatment pattern changes.</p><p><strong>Methods: </strong>This single-center, retrospective, IRB-approved study at MSKCC included patients with immunocompetent PCNSL, age ≥18 years and diagnosed between 1/1983-12/2017. Overall survival (OS) was modeled from date of last HDMTX for analyses associating HDMTX and OS. Multivariable Cox regression models estimated hazard ratios (HR) and corresponding 95% confidence intervals (CI).</p><p><strong>Results: </strong>There were 546 patients identified with newly diagnosed PCNSL. Median overall survival (mOS) of the entire population was 4.7 years (95% CI: 3.8-5.7 years); 3.3 years (95% CI: 2.7-3.9 years) in patients diagnosed prior to 2006 and 8.1 years (95% CI: 6.6-11.1 years) in patients diagnosed 2006 onwards. Patients receiving ≥6 doses of HDMTX had improved survival compared to those receiving <6 doses of HDMTX (mOS: 7.8 <i>vs.</i> 4.3 years; P=0.001). Patients receiving induction rituximab had improved OS compared to those who did not receive rituximab (mOS: 10.5 <i>vs.</i> 3.2 years; P<0.0001). Patients receiving ≥6 doses of HDMTX and rituximab had greatest mOS at 13 years, with a 70% reduction in death (HR =0.30; 95% CI: 0.19-0.47) adjusting for treatment era, sex, and recursive partitioning analysis (RPA) classes comprising age and karnofsky performance score (KPS).</p><p><strong>Conclusions: </strong>OS for PCNSL has improved significantly over the last few decades. Patients seem to benefit with ≥6 doses of HDMTX and the addition of rituximab, an effect independent of treatment era, age, and KPS.</p>","PeriodicalId":72224,"journal":{"name":"Annals of lymphoma","volume":"7 ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-02-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/34/8c/nihms-1887687.PMC10100595.pdf","citationCount":"2","resultStr":"{\"title\":\"Is more better? Increased doses of high dose methotrexate and addition of rituximab is associated with improved outcomes in a large primary CNS lymphoma cohort.\",\"authors\":\"Prakirthi Yerram, Samantha N Reiss, Lisa Modelevsky, Lauren Schaff, Anne S Reiner, Katherine S Panageas, Christian Grommes\",\"doi\":\"10.21037/aol-22-19\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Primary central nervous system lymphoma (PCNSL) is a rare and aggressive primary brain tumor. While high dose methotrexate (HDMTX) regimens remain standard of care, it remains unclear if optimization of HDMTX doses and the addition of rituximab provide clinical benefit. Over the last 30 years, standard care given at Memorial Sloan Kettering Cancer Center (MSKCC) has evolved, allowing the comparison of patients receiving different numbers of HDMTX doses and those treated with and without rituximab. The purpose of this study was to describe outcomes based on treatment pattern changes.</p><p><strong>Methods: </strong>This single-center, retrospective, IRB-approved study at MSKCC included patients with immunocompetent PCNSL, age ≥18 years and diagnosed between 1/1983-12/2017. Overall survival (OS) was modeled from date of last HDMTX for analyses associating HDMTX and OS. Multivariable Cox regression models estimated hazard ratios (HR) and corresponding 95% confidence intervals (CI).</p><p><strong>Results: </strong>There were 546 patients identified with newly diagnosed PCNSL. Median overall survival (mOS) of the entire population was 4.7 years (95% CI: 3.8-5.7 years); 3.3 years (95% CI: 2.7-3.9 years) in patients diagnosed prior to 2006 and 8.1 years (95% CI: 6.6-11.1 years) in patients diagnosed 2006 onwards. Patients receiving ≥6 doses of HDMTX had improved survival compared to those receiving <6 doses of HDMTX (mOS: 7.8 <i>vs.</i> 4.3 years; P=0.001). Patients receiving induction rituximab had improved OS compared to those who did not receive rituximab (mOS: 10.5 <i>vs.</i> 3.2 years; P<0.0001). Patients receiving ≥6 doses of HDMTX and rituximab had greatest mOS at 13 years, with a 70% reduction in death (HR =0.30; 95% CI: 0.19-0.47) adjusting for treatment era, sex, and recursive partitioning analysis (RPA) classes comprising age and karnofsky performance score (KPS).</p><p><strong>Conclusions: </strong>OS for PCNSL has improved significantly over the last few decades. Patients seem to benefit with ≥6 doses of HDMTX and the addition of rituximab, an effect independent of treatment era, age, and KPS.</p>\",\"PeriodicalId\":72224,\"journal\":{\"name\":\"Annals of lymphoma\",\"volume\":\"7 \",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-02-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/34/8c/nihms-1887687.PMC10100595.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of lymphoma\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.21037/aol-22-19\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of lymphoma","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/aol-22-19","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Is more better? Increased doses of high dose methotrexate and addition of rituximab is associated with improved outcomes in a large primary CNS lymphoma cohort.
Background: Primary central nervous system lymphoma (PCNSL) is a rare and aggressive primary brain tumor. While high dose methotrexate (HDMTX) regimens remain standard of care, it remains unclear if optimization of HDMTX doses and the addition of rituximab provide clinical benefit. Over the last 30 years, standard care given at Memorial Sloan Kettering Cancer Center (MSKCC) has evolved, allowing the comparison of patients receiving different numbers of HDMTX doses and those treated with and without rituximab. The purpose of this study was to describe outcomes based on treatment pattern changes.
Methods: This single-center, retrospective, IRB-approved study at MSKCC included patients with immunocompetent PCNSL, age ≥18 years and diagnosed between 1/1983-12/2017. Overall survival (OS) was modeled from date of last HDMTX for analyses associating HDMTX and OS. Multivariable Cox regression models estimated hazard ratios (HR) and corresponding 95% confidence intervals (CI).
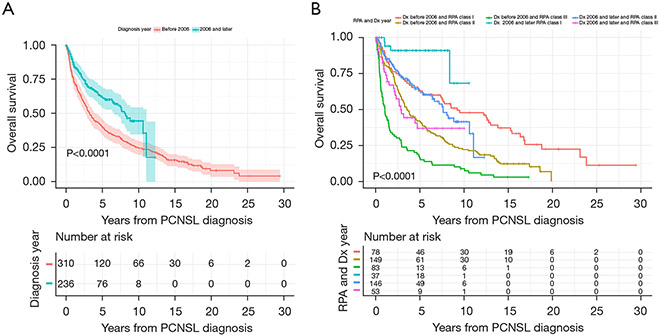
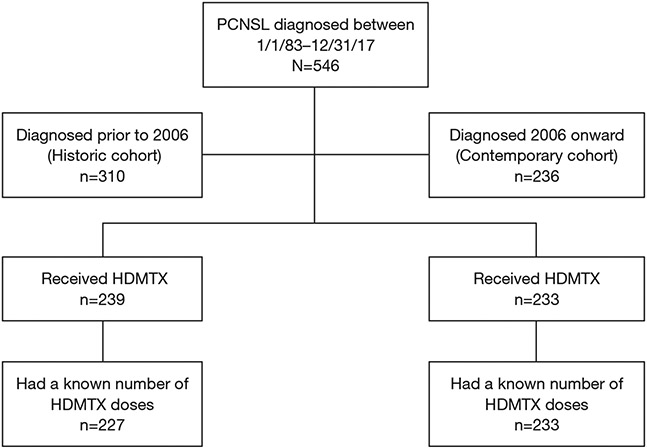
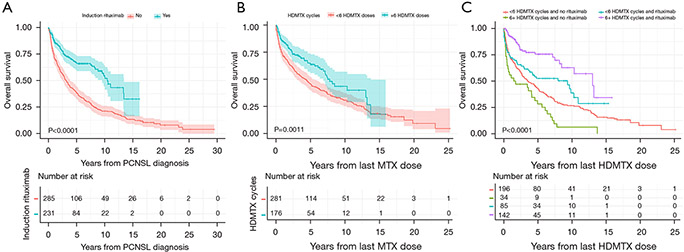
Results: There were 546 patients identified with newly diagnosed PCNSL. Median overall survival (mOS) of the entire population was 4.7 years (95% CI: 3.8-5.7 years); 3.3 years (95% CI: 2.7-3.9 years) in patients diagnosed prior to 2006 and 8.1 years (95% CI: 6.6-11.1 years) in patients diagnosed 2006 onwards. Patients receiving ≥6 doses of HDMTX had improved survival compared to those receiving <6 doses of HDMTX (mOS: 7.8 vs. 4.3 years; P=0.001). Patients receiving induction rituximab had improved OS compared to those who did not receive rituximab (mOS: 10.5 vs. 3.2 years; P<0.0001). Patients receiving ≥6 doses of HDMTX and rituximab had greatest mOS at 13 years, with a 70% reduction in death (HR =0.30; 95% CI: 0.19-0.47) adjusting for treatment era, sex, and recursive partitioning analysis (RPA) classes comprising age and karnofsky performance score (KPS).
Conclusions: OS for PCNSL has improved significantly over the last few decades. Patients seem to benefit with ≥6 doses of HDMTX and the addition of rituximab, an effect independent of treatment era, age, and KPS.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


