{"title":"13岁男孩肾盂成形术失败后输尿管上段以锥形降结肠重建一例。","authors":"Hideaki Nakajima, Hiroyuki Koga, Seitaro Kosaka, Mao Ikari, Geoffrey J Lane, Atsuyuki Yamataka","doi":"10.1055/a-2035-4637","DOIUrl":null,"url":null,"abstract":"<p><p>An 11-year-old boy was referred for further management of a 6-cm-long grossly stenosed ureter following two failed left ureteropelvic junction (UPJ) obstruction repairs elsewhere. A tapered segment of the descending colon (TDC) was used successfully for ureteral reconstruction. The UPJ was exposed through a left flank incision. The stenosed segment was excised; both ends appeared severely inflamed and thickened. Tissue interposition was required and ureteroplasty with a TDC was performed by incising the peritoneum adjacent to the excised ureter to mobilize the descending colon to the retroperitoneal space. To prepare the TDC, an 8-cm segment of the colon with intact blood vessels was isolated, tapered, and sutured into a funnel shape using a 14-Fr catheter as a temporary stent. After colocolostomy, the colon was returned to the abdominal cavity, the peritoneum was closed carefully to prevent vascular compromise, and the TDC was anastomosed to the ureter and renal calyx with interrupted absorbable sutures. A double J stent (DJS) and percutaneous nephrostomy tube were placed. Postoperative recovery was uneventful. The DJS was removed on day 50 after confirming smooth urine flow through both the ureter-TDC and calyx-TDC anastomoses. Diuretic renography performed 68 days postoperatively was unobstructed. The patient is currently well after 12 months follow-up. This would appear to be the first report of a TDC being used to create a funnel-shaped segment to reconstruct a long, grossly stenosed ureter. The TDC is simpler than the re-tubularizing colon but requires monitoring for postoperative mucus-related complications and malignant transformation.</p>","PeriodicalId":43204,"journal":{"name":"European Journal of Pediatric Surgery Reports","volume":"11 1","pages":"e10-e14"},"PeriodicalIF":0.7000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10085642/pdf/","citationCount":"0","resultStr":"{\"title\":\"Upper Ureteral Reconstruction with a Tapered Descending Colon after Failed Pyeloplasties in a 13-Year-Old Boy.\",\"authors\":\"Hideaki Nakajima, Hiroyuki Koga, Seitaro Kosaka, Mao Ikari, Geoffrey J Lane, Atsuyuki Yamataka\",\"doi\":\"10.1055/a-2035-4637\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>An 11-year-old boy was referred for further management of a 6-cm-long grossly stenosed ureter following two failed left ureteropelvic junction (UPJ) obstruction repairs elsewhere. A tapered segment of the descending colon (TDC) was used successfully for ureteral reconstruction. The UPJ was exposed through a left flank incision. The stenosed segment was excised; both ends appeared severely inflamed and thickened. Tissue interposition was required and ureteroplasty with a TDC was performed by incising the peritoneum adjacent to the excised ureter to mobilize the descending colon to the retroperitoneal space. To prepare the TDC, an 8-cm segment of the colon with intact blood vessels was isolated, tapered, and sutured into a funnel shape using a 14-Fr catheter as a temporary stent. After colocolostomy, the colon was returned to the abdominal cavity, the peritoneum was closed carefully to prevent vascular compromise, and the TDC was anastomosed to the ureter and renal calyx with interrupted absorbable sutures. A double J stent (DJS) and percutaneous nephrostomy tube were placed. Postoperative recovery was uneventful. The DJS was removed on day 50 after confirming smooth urine flow through both the ureter-TDC and calyx-TDC anastomoses. Diuretic renography performed 68 days postoperatively was unobstructed. The patient is currently well after 12 months follow-up. This would appear to be the first report of a TDC being used to create a funnel-shaped segment to reconstruct a long, grossly stenosed ureter. The TDC is simpler than the re-tubularizing colon but requires monitoring for postoperative mucus-related complications and malignant transformation.</p>\",\"PeriodicalId\":43204,\"journal\":{\"name\":\"European Journal of Pediatric Surgery Reports\",\"volume\":\"11 1\",\"pages\":\"e10-e14\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10085642/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Pediatric Surgery Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/a-2035-4637\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Pediatric Surgery Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-2035-4637","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
Upper Ureteral Reconstruction with a Tapered Descending Colon after Failed Pyeloplasties in a 13-Year-Old Boy.
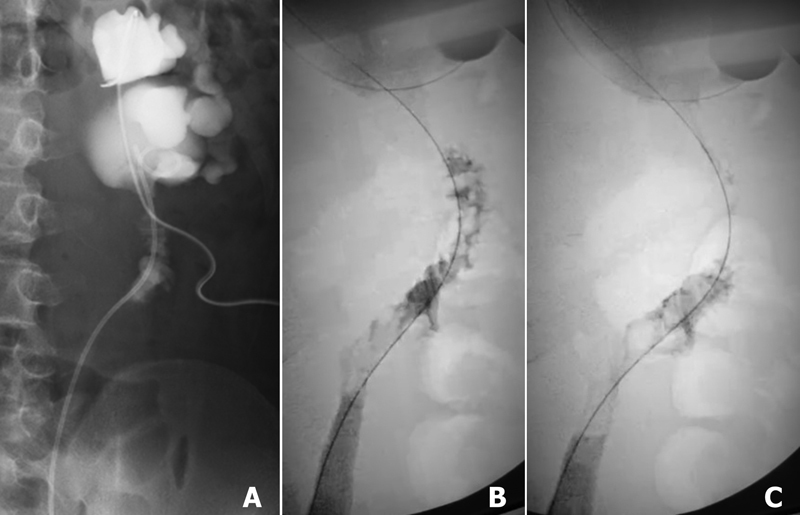
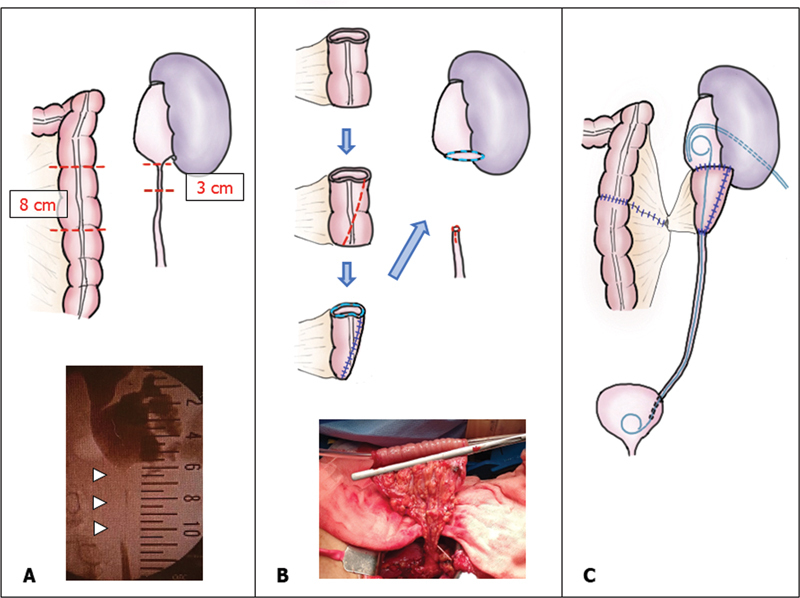
An 11-year-old boy was referred for further management of a 6-cm-long grossly stenosed ureter following two failed left ureteropelvic junction (UPJ) obstruction repairs elsewhere. A tapered segment of the descending colon (TDC) was used successfully for ureteral reconstruction. The UPJ was exposed through a left flank incision. The stenosed segment was excised; both ends appeared severely inflamed and thickened. Tissue interposition was required and ureteroplasty with a TDC was performed by incising the peritoneum adjacent to the excised ureter to mobilize the descending colon to the retroperitoneal space. To prepare the TDC, an 8-cm segment of the colon with intact blood vessels was isolated, tapered, and sutured into a funnel shape using a 14-Fr catheter as a temporary stent. After colocolostomy, the colon was returned to the abdominal cavity, the peritoneum was closed carefully to prevent vascular compromise, and the TDC was anastomosed to the ureter and renal calyx with interrupted absorbable sutures. A double J stent (DJS) and percutaneous nephrostomy tube were placed. Postoperative recovery was uneventful. The DJS was removed on day 50 after confirming smooth urine flow through both the ureter-TDC and calyx-TDC anastomoses. Diuretic renography performed 68 days postoperatively was unobstructed. The patient is currently well after 12 months follow-up. This would appear to be the first report of a TDC being used to create a funnel-shaped segment to reconstruct a long, grossly stenosed ureter. The TDC is simpler than the re-tubularizing colon but requires monitoring for postoperative mucus-related complications and malignant transformation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


