Basit A Azizi, Ricardo Munoz-Acuna, Aiman Suleiman, Elena Ahrens, Simone Redaelli, Tim M Tartler, Guanqing Chen, Boris Jung, Daniel Talmor, Elias N Baedorf-Kassis, Maximilian S Schaefer
{"title":"2019年冠状病毒病和非冠状病毒病机械通气危重患者的机械功率和30天死亡率:一项医院登记研究","authors":"Basit A Azizi, Ricardo Munoz-Acuna, Aiman Suleiman, Elena Ahrens, Simone Redaelli, Tim M Tartler, Guanqing Chen, Boris Jung, Daniel Talmor, Elias N Baedorf-Kassis, Maximilian S Schaefer","doi":"10.1186/s40560-023-00662-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Previous studies linked a high intensity of ventilation, measured as mechanical power, to mortality in patients suffering from \"classic\" ARDS. By contrast, mechanically ventilated patients with a diagnosis of COVID-19 may present with intact pulmonary mechanics while undergoing mechanical ventilation for longer periods of time. We investigated whether an association between higher mechanical power and mortality is modified by a diagnosis of COVID-19.</p><p><strong>Methods: </strong>This retrospective study included critically ill, adult patients who were mechanically ventilated for at least 24 h between March 2020 and December 2021 at a tertiary healthcare facility in Boston, Massachusetts. The primary exposure was median mechanical power during the first 24 h of mechanical ventilation, calculated using a previously validated formula. The primary outcome was 30-day mortality. As co-primary analysis, we investigated whether a diagnosis of COVID-19 modified the primary association. We further investigated the association between mechanical power and days being alive and ventilator free and effect modification of this by a diagnosis of COVID-19. Multivariable logistic regression, effect modification and negative binomial regression analyses adjusted for baseline patient characteristics, severity of disease and in-hospital factors, were applied.</p><p><strong>Results: </strong>1,737 mechanically ventilated patients were included, 411 (23.7%) suffered from COVID-19. 509 (29.3%) died within 30 days. The median mechanical power during the first 24 h of ventilation was 19.3 [14.6-24.0] J/min in patients with and 13.2 [10.2-18.0] J/min in patients without COVID-19. A higher mechanical power was associated with 30-day mortality (OR<sub>adj</sub> 1.26 per 1-SD, 7.1J/min increase; 95% CI 1.09-1.46; p = 0.002). Effect modification and interaction analysis did not support that this association was modified by a diagnosis of COVID-19 (95% CI, 0.81-1.38; p-for-interaction = 0.68). A higher mechanical power was associated with a lower number of days alive and ventilator free until day 28 (IRR<sub>adj</sub> 0.83 per 7.1 J/min increase; 95% CI 0.75-0.91; p < 0.001, adjusted risk difference - 2.7 days per 7.1J/min increase; 95% CI - 4.1 to - 1.3).</p><p><strong>Conclusion: </strong>A higher mechanical power is associated with elevated 30-day mortality. While patients with COVID-19 received mechanical ventilation with higher mechanical power, this association was independent of a concomitant diagnosis of COVID-19.</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":"11 1","pages":"14"},"PeriodicalIF":3.8000,"publicationDate":"2023-04-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10077655/pdf/","citationCount":"1","resultStr":"{\"title\":\"Mechanical power and 30-day mortality in mechanically ventilated, critically ill patients with and without Coronavirus Disease-2019: a hospital registry study.\",\"authors\":\"Basit A Azizi, Ricardo Munoz-Acuna, Aiman Suleiman, Elena Ahrens, Simone Redaelli, Tim M Tartler, Guanqing Chen, Boris Jung, Daniel Talmor, Elias N Baedorf-Kassis, Maximilian S Schaefer\",\"doi\":\"10.1186/s40560-023-00662-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Previous studies linked a high intensity of ventilation, measured as mechanical power, to mortality in patients suffering from \\\"classic\\\" ARDS. By contrast, mechanically ventilated patients with a diagnosis of COVID-19 may present with intact pulmonary mechanics while undergoing mechanical ventilation for longer periods of time. We investigated whether an association between higher mechanical power and mortality is modified by a diagnosis of COVID-19.</p><p><strong>Methods: </strong>This retrospective study included critically ill, adult patients who were mechanically ventilated for at least 24 h between March 2020 and December 2021 at a tertiary healthcare facility in Boston, Massachusetts. The primary exposure was median mechanical power during the first 24 h of mechanical ventilation, calculated using a previously validated formula. The primary outcome was 30-day mortality. As co-primary analysis, we investigated whether a diagnosis of COVID-19 modified the primary association. We further investigated the association between mechanical power and days being alive and ventilator free and effect modification of this by a diagnosis of COVID-19. Multivariable logistic regression, effect modification and negative binomial regression analyses adjusted for baseline patient characteristics, severity of disease and in-hospital factors, were applied.</p><p><strong>Results: </strong>1,737 mechanically ventilated patients were included, 411 (23.7%) suffered from COVID-19. 509 (29.3%) died within 30 days. The median mechanical power during the first 24 h of ventilation was 19.3 [14.6-24.0] J/min in patients with and 13.2 [10.2-18.0] J/min in patients without COVID-19. A higher mechanical power was associated with 30-day mortality (OR<sub>adj</sub> 1.26 per 1-SD, 7.1J/min increase; 95% CI 1.09-1.46; p = 0.002). Effect modification and interaction analysis did not support that this association was modified by a diagnosis of COVID-19 (95% CI, 0.81-1.38; p-for-interaction = 0.68). A higher mechanical power was associated with a lower number of days alive and ventilator free until day 28 (IRR<sub>adj</sub> 0.83 per 7.1 J/min increase; 95% CI 0.75-0.91; p < 0.001, adjusted risk difference - 2.7 days per 7.1J/min increase; 95% CI - 4.1 to - 1.3).</p><p><strong>Conclusion: </strong>A higher mechanical power is associated with elevated 30-day mortality. While patients with COVID-19 received mechanical ventilation with higher mechanical power, this association was independent of a concomitant diagnosis of COVID-19.</p>\",\"PeriodicalId\":16123,\"journal\":{\"name\":\"Journal of Intensive Care\",\"volume\":\"11 1\",\"pages\":\"14\"},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2023-04-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10077655/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Intensive Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s40560-023-00662-7\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-023-00662-7","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 1
摘要
背景:先前的研究将高强度的通气(以机械功率衡量)与“典型”ARDS患者的死亡率联系起来。相比之下,诊断为COVID-19的机械通气患者在进行机械通气的时间较长时,肺力学可能完好无损。我们调查了高机械功率与死亡率之间的关联是否会因COVID-19的诊断而改变。方法:这项回顾性研究纳入了2020年3月至2021年12月期间在马萨诸塞州波士顿一家三级医疗机构接受机械通气至少24小时的危重症成年患者。主要暴露是机械通气前24小时的中位机械功率,使用先前验证的公式计算。主要终点为30天死亡率。作为共同主要分析,我们调查了COVID-19的诊断是否改变了主要关联。我们进一步调查了机械功率与存活天数和无呼吸机之间的关系,以及诊断为COVID-19后对这种关系的影响。应用多变量logistic回归、效应修正和负二项回归分析,调整基线患者特征、疾病严重程度和院内因素。结果:纳入机械通气患者1737例,新冠肺炎患者411例(23.7%)。509例(29.3%)在30天内死亡。新冠肺炎患者通气前24 h机械功率中位数为19.3 [14.6-24.0]J/min,非新冠肺炎患者为13.2 [10.2-18.0]J/min。较高的机械功率与30天死亡率相关(ORadj 1.26 / 1-SD,增加7.1J/min;95% ci 1.09-1.46;p = 0.002)。效应修正和相互作用分析不支持这种关联被COVID-19的诊断所修正(95% CI, 0.81-1.38;p-for-interaction = 0.68)。较高的机械功率与存活天数和28天前无呼吸机天数相关(IRRadj为0.83 / 7.1 J/min;95% ci 0.75-0.91;p结论:较高的机械功率与较高的30天死亡率相关。虽然COVID-19患者接受更高机械功率的机械通气,但这种关联与伴随的COVID-19诊断无关。
Mechanical power and 30-day mortality in mechanically ventilated, critically ill patients with and without Coronavirus Disease-2019: a hospital registry study.
Background: Previous studies linked a high intensity of ventilation, measured as mechanical power, to mortality in patients suffering from "classic" ARDS. By contrast, mechanically ventilated patients with a diagnosis of COVID-19 may present with intact pulmonary mechanics while undergoing mechanical ventilation for longer periods of time. We investigated whether an association between higher mechanical power and mortality is modified by a diagnosis of COVID-19.
Methods: This retrospective study included critically ill, adult patients who were mechanically ventilated for at least 24 h between March 2020 and December 2021 at a tertiary healthcare facility in Boston, Massachusetts. The primary exposure was median mechanical power during the first 24 h of mechanical ventilation, calculated using a previously validated formula. The primary outcome was 30-day mortality. As co-primary analysis, we investigated whether a diagnosis of COVID-19 modified the primary association. We further investigated the association between mechanical power and days being alive and ventilator free and effect modification of this by a diagnosis of COVID-19. Multivariable logistic regression, effect modification and negative binomial regression analyses adjusted for baseline patient characteristics, severity of disease and in-hospital factors, were applied.
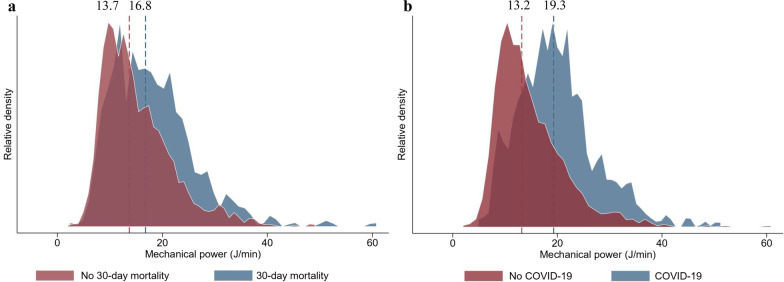
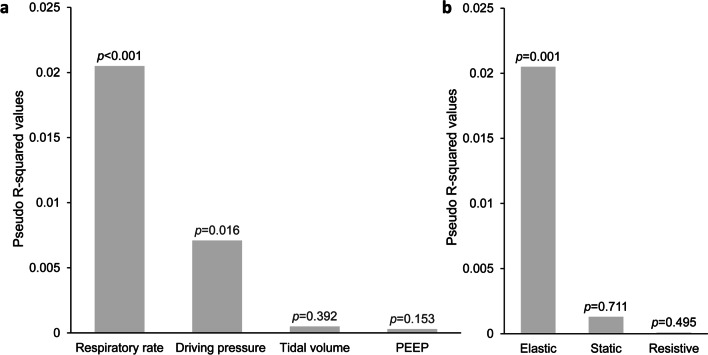
Results: 1,737 mechanically ventilated patients were included, 411 (23.7%) suffered from COVID-19. 509 (29.3%) died within 30 days. The median mechanical power during the first 24 h of ventilation was 19.3 [14.6-24.0] J/min in patients with and 13.2 [10.2-18.0] J/min in patients without COVID-19. A higher mechanical power was associated with 30-day mortality (ORadj 1.26 per 1-SD, 7.1J/min increase; 95% CI 1.09-1.46; p = 0.002). Effect modification and interaction analysis did not support that this association was modified by a diagnosis of COVID-19 (95% CI, 0.81-1.38; p-for-interaction = 0.68). A higher mechanical power was associated with a lower number of days alive and ventilator free until day 28 (IRRadj 0.83 per 7.1 J/min increase; 95% CI 0.75-0.91; p < 0.001, adjusted risk difference - 2.7 days per 7.1J/min increase; 95% CI - 4.1 to - 1.3).
Conclusion: A higher mechanical power is associated with elevated 30-day mortality. While patients with COVID-19 received mechanical ventilation with higher mechanical power, this association was independent of a concomitant diagnosis of COVID-19.
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


