Alexander Booth, Henry Colorado, Gayenell Magwood, Erin Forster, Robert N Axon, Thomas Curran
{"title":"远离家乡:旅行距离和护理碎片在炎症性肠病手术结果中的作用。","authors":"Alexander Booth, Henry Colorado, Gayenell Magwood, Erin Forster, Robert N Axon, Thomas Curran","doi":"10.1093/crocol/otad015","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Fragmented care for inflammatory bowel disease (IBD) is known to correlate negatively with outcomes, but it is unclear which aspects of care fragmentation are relevant and potentially modifiable. Furthermore, there is little data on the relationship between travel distance and the benefits of integrated care models. Hypothesizing care coordination in the preoperative period may have a significant impact on surgical outcomes, we explored associations between integrated care, travel distance, and surgical outcomes.</p><p><strong>Methods: </strong>A single-center retrospective cohort study of patients undergoing index abdominal surgery was done to compare the rate of surgical complications with and without long travel distance and nonintegrated preoperative care. Multivariable logistic regression was used to identify factors independently associated with complications.</p><p><strong>Results: </strong>One hundred and fifty-seven patients were included. Complications were more common among patients with travel distance >75 miles (47.6% vs 27.4%, <i>P</i> = .012). Integrated preoperative care was not significant on bivariate (<i>P</i> = .381) or multivariable analysis but had a stronger association among patients with travel distance <75 miles (20.9% integrated vs 36.7%, <i>P</i> = .138). After adjustment, new ileostomy, open surgical approach, and distance >75 miles were independently associated with complications.</p><p><strong>Conclusions: </strong>Patients with longer travel distances to the hospital were twice as likely to have a surgical complication after adjusting for other risk factors. Without significant accommodations for remote patients, potential benefits of an integrated model for IBD care may be limited to patients who live close to the medical center. Future efforts addressing continuity of care should consider tactics to mitigate the impact of travel distance on outcomes.</p>","PeriodicalId":10847,"journal":{"name":"Crohn's & Colitis 360","volume":"5 2","pages":"otad015"},"PeriodicalIF":1.8000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/bb/5f/otad015.PMC10066839.pdf","citationCount":"0","resultStr":"{\"title\":\"Far From Home: The Role of Travel Distance and Care Fragmentation in Surgical Outcomes for Inflammatory Bowel Disease.\",\"authors\":\"Alexander Booth, Henry Colorado, Gayenell Magwood, Erin Forster, Robert N Axon, Thomas Curran\",\"doi\":\"10.1093/crocol/otad015\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Fragmented care for inflammatory bowel disease (IBD) is known to correlate negatively with outcomes, but it is unclear which aspects of care fragmentation are relevant and potentially modifiable. Furthermore, there is little data on the relationship between travel distance and the benefits of integrated care models. Hypothesizing care coordination in the preoperative period may have a significant impact on surgical outcomes, we explored associations between integrated care, travel distance, and surgical outcomes.</p><p><strong>Methods: </strong>A single-center retrospective cohort study of patients undergoing index abdominal surgery was done to compare the rate of surgical complications with and without long travel distance and nonintegrated preoperative care. Multivariable logistic regression was used to identify factors independently associated with complications.</p><p><strong>Results: </strong>One hundred and fifty-seven patients were included. Complications were more common among patients with travel distance >75 miles (47.6% vs 27.4%, <i>P</i> = .012). Integrated preoperative care was not significant on bivariate (<i>P</i> = .381) or multivariable analysis but had a stronger association among patients with travel distance <75 miles (20.9% integrated vs 36.7%, <i>P</i> = .138). After adjustment, new ileostomy, open surgical approach, and distance >75 miles were independently associated with complications.</p><p><strong>Conclusions: </strong>Patients with longer travel distances to the hospital were twice as likely to have a surgical complication after adjusting for other risk factors. Without significant accommodations for remote patients, potential benefits of an integrated model for IBD care may be limited to patients who live close to the medical center. Future efforts addressing continuity of care should consider tactics to mitigate the impact of travel distance on outcomes.</p>\",\"PeriodicalId\":10847,\"journal\":{\"name\":\"Crohn's & Colitis 360\",\"volume\":\"5 2\",\"pages\":\"otad015\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2023-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/bb/5f/otad015.PMC10066839.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Crohn's & Colitis 360\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/crocol/otad015\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Crohn's & Colitis 360","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/crocol/otad015","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
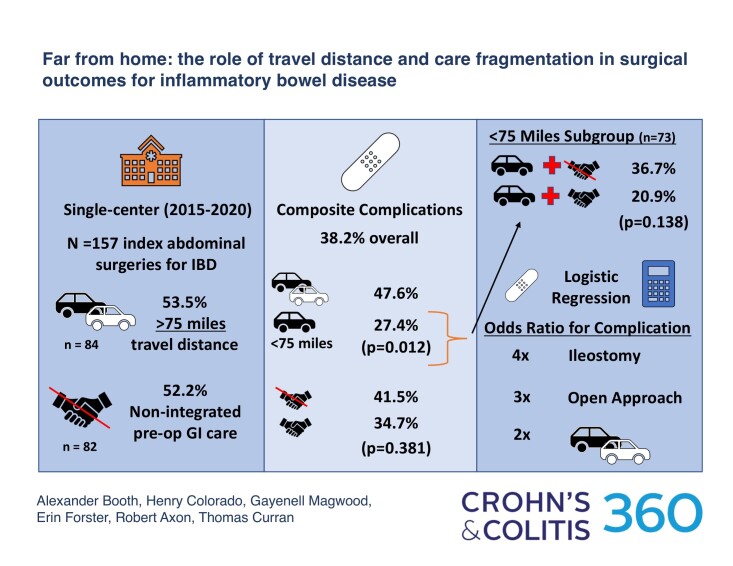
背景:众所周知,炎症性肠病(IBD)的碎片化护理与预后呈负相关,但尚不清楚护理碎片化的哪些方面是相关的,哪些方面可能是可以改变的。此外,关于出行距离与综合护理模式效益之间关系的数据很少。假设术前护理协调可能对手术结果有显著影响,我们探讨了综合护理、旅行距离和手术结果之间的关系。方法:采用单中心回顾性队列研究方法,对腹部手术患者进行回顾性研究,比较有无长距离手术和术前非综合护理的手术并发症发生率。使用多变量逻辑回归来确定与并发症独立相关的因素。结果:纳入157例患者。旅行距离>75英里的患者并发症更为常见(47.6% vs 27.4%, P = 0.012)。综合术前护理在双变量分析(P = .381)或多变量分析中均无显著性差异,但与患者出行距离的相关性较强(P = .138)。调整后,新的回肠造口、开放手术入路和距离>75英里与并发症独立相关。结论:在调整其他危险因素后,到医院路程较长的患者发生手术并发症的可能性是其他危险因素的两倍。如果没有为偏远地区的患者提供显著的便利,IBD综合治疗模式的潜在益处可能仅限于居住在医疗中心附近的患者。未来解决护理连续性问题的努力应考虑减轻旅行距离对结果影响的策略。
Far From Home: The Role of Travel Distance and Care Fragmentation in Surgical Outcomes for Inflammatory Bowel Disease.
Background: Fragmented care for inflammatory bowel disease (IBD) is known to correlate negatively with outcomes, but it is unclear which aspects of care fragmentation are relevant and potentially modifiable. Furthermore, there is little data on the relationship between travel distance and the benefits of integrated care models. Hypothesizing care coordination in the preoperative period may have a significant impact on surgical outcomes, we explored associations between integrated care, travel distance, and surgical outcomes.
Methods: A single-center retrospective cohort study of patients undergoing index abdominal surgery was done to compare the rate of surgical complications with and without long travel distance and nonintegrated preoperative care. Multivariable logistic regression was used to identify factors independently associated with complications.
Results: One hundred and fifty-seven patients were included. Complications were more common among patients with travel distance >75 miles (47.6% vs 27.4%, P = .012). Integrated preoperative care was not significant on bivariate (P = .381) or multivariable analysis but had a stronger association among patients with travel distance <75 miles (20.9% integrated vs 36.7%, P = .138). After adjustment, new ileostomy, open surgical approach, and distance >75 miles were independently associated with complications.
Conclusions: Patients with longer travel distances to the hospital were twice as likely to have a surgical complication after adjusting for other risk factors. Without significant accommodations for remote patients, potential benefits of an integrated model for IBD care may be limited to patients who live close to the medical center. Future efforts addressing continuity of care should consider tactics to mitigate the impact of travel distance on outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


