Alex M Cressman, Ushma Purohit, Ellen Shadowitz, Edward Etchells, Adina Weinerman, Darren Gerson, Kaveh G Shojania, Lynfa Stroud, Brian M Wong, Steve Shadowitz
{"title":"学术教学医院普通内科潜在可避免的入院:一项观察性研究。","authors":"Alex M Cressman, Ushma Purohit, Ellen Shadowitz, Edward Etchells, Adina Weinerman, Darren Gerson, Kaveh G Shojania, Lynfa Stroud, Brian M Wong, Steve Shadowitz","doi":"10.9778/cmajo.20220020","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Identifying potentially avoidable admissions to Canadian hospitals is an important health system goal. With general internal medicine (GIM) accounting for 40% of hospital admissions, we sought to develop a method to identify potentially avoidable admissions and characterize patient, provider and health system factors.</p><p><strong>Methods: </strong>We conducted an observational study of GIM admissions at our institution from August 2019 to February 2020. We defined potentially avoidable admissions as admissions that could be managed in an appropriate and safe manner in the emergency department or ambulatory setting and asked staff physicians to screen admissions daily and flag candidates as potentially avoidable admissions. For each candidate, we prepared a case review and debriefed with members of the admitting team. We then reviewed each candidate with our research team, assigned an avoidability score (1 [low] to 4 [high]) and identified contributing factors for those with scores of 3 or more.</p><p><strong>Results: </strong>We screened 601 total admissions and staff physicians flagged 117 (19.5%) of these as candidate potential avoidable admissions. Consensus review identified 67 candidates as potentially avoidable admissions (11.1%, 95% confidence interval 8.8%-13.9%); these patients were younger (mean age 65 yr v. 72 yr), had fewer comorbidities (Canadian Institute for Health Information Case Mix Group+ 0.42 v. 1.14), had lower resource-intensity weighting scores (0.72 v. 1.50) and shorter hospital lengths of stay (29 h v. 105 h) (<i>p</i> < 0.01). Common factors included diagnostic and therapeutic uncertainty, perceived need for short-term monitoring, government directive of a 4-hour limit for admission decision-making and subspecialist request to admit.</p><p><strong>Interpretation: </strong>Our prospective method of screening, flagging and case review showed that 1 in 9 GIM admissions were potentially avoidable. Other institutions could consider adapting this methodology to ascertain their rate of potentially avoidable admissions and to understand contributing factors to inform improvement endeavours.</p>","PeriodicalId":10432,"journal":{"name":"CMAJ open","volume":"11 1","pages":"E201-E207"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/77/5a/cmajo.20220020.PMC9981162.pdf","citationCount":"0","resultStr":"{\"title\":\"Potentially avoidable admissions to general internal medicine at an academic teaching hospital: an observational study.\",\"authors\":\"Alex M Cressman, Ushma Purohit, Ellen Shadowitz, Edward Etchells, Adina Weinerman, Darren Gerson, Kaveh G Shojania, Lynfa Stroud, Brian M Wong, Steve Shadowitz\",\"doi\":\"10.9778/cmajo.20220020\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Identifying potentially avoidable admissions to Canadian hospitals is an important health system goal. With general internal medicine (GIM) accounting for 40% of hospital admissions, we sought to develop a method to identify potentially avoidable admissions and characterize patient, provider and health system factors.</p><p><strong>Methods: </strong>We conducted an observational study of GIM admissions at our institution from August 2019 to February 2020. We defined potentially avoidable admissions as admissions that could be managed in an appropriate and safe manner in the emergency department or ambulatory setting and asked staff physicians to screen admissions daily and flag candidates as potentially avoidable admissions. For each candidate, we prepared a case review and debriefed with members of the admitting team. We then reviewed each candidate with our research team, assigned an avoidability score (1 [low] to 4 [high]) and identified contributing factors for those with scores of 3 or more.</p><p><strong>Results: </strong>We screened 601 total admissions and staff physicians flagged 117 (19.5%) of these as candidate potential avoidable admissions. Consensus review identified 67 candidates as potentially avoidable admissions (11.1%, 95% confidence interval 8.8%-13.9%); these patients were younger (mean age 65 yr v. 72 yr), had fewer comorbidities (Canadian Institute for Health Information Case Mix Group+ 0.42 v. 1.14), had lower resource-intensity weighting scores (0.72 v. 1.50) and shorter hospital lengths of stay (29 h v. 105 h) (<i>p</i> < 0.01). Common factors included diagnostic and therapeutic uncertainty, perceived need for short-term monitoring, government directive of a 4-hour limit for admission decision-making and subspecialist request to admit.</p><p><strong>Interpretation: </strong>Our prospective method of screening, flagging and case review showed that 1 in 9 GIM admissions were potentially avoidable. Other institutions could consider adapting this methodology to ascertain their rate of potentially avoidable admissions and to understand contributing factors to inform improvement endeavours.</p>\",\"PeriodicalId\":10432,\"journal\":{\"name\":\"CMAJ open\",\"volume\":\"11 1\",\"pages\":\"E201-E207\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/77/5a/cmajo.20220020.PMC9981162.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"CMAJ open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.9778/cmajo.20220020\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"CMAJ open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.9778/cmajo.20220020","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:确定潜在的可避免的入院加拿大医院是一个重要的卫生系统的目标。由于普通内科(GIM)占住院人数的40%,我们试图开发一种方法来确定潜在的可避免的住院,并表征患者,提供者和卫生系统因素。方法:我们对我院2019年8月至2020年2月的GIM入学情况进行了观察性研究。我们将潜在可避免入院定义为可在急诊科或门诊环境中以适当和安全的方式进行管理的入院,并要求工作医师每天筛选入院患者,并将候选人标记为潜在可避免入院。对于每个候选人,我们都准备了一份案例回顾,并与录取小组的成员进行了汇报。然后我们和我们的研究团队对每个候选人进行了评估,分配了一个可避免性得分(1[低]到4[高]),并确定了得分为3分或以上的人的影响因素。结果:我们筛选了601例住院患者,工作人员医生将其中117例(19.5%)标记为候选潜在可避免的住院患者。共识审查确定了67名候选人可能可以避免入学(11.1%,95%置信区间8.8%-13.9%);这些患者更年轻(平均年龄65岁vs 72岁),合合症更少(加拿大卫生信息研究所病例混合组+ 0.42 vs 1.14),资源强度加权评分更低(0.72 vs 1.50),住院时间更短(29 h vs 105 h) (p < 0.01)。常见的因素包括诊断和治疗的不确定性,认为需要短期监测,政府指示4小时的入院决策限制和专科医生的入院请求。解释:我们的前瞻性筛查、标记和病例回顾方法显示,1 / 9的GIM入院是可以避免的。其他院校可考虑采用此方法,以确定其可避免的入学率,并了解影响因素,为改善工作提供信息。
Potentially avoidable admissions to general internal medicine at an academic teaching hospital: an observational study.
Background: Identifying potentially avoidable admissions to Canadian hospitals is an important health system goal. With general internal medicine (GIM) accounting for 40% of hospital admissions, we sought to develop a method to identify potentially avoidable admissions and characterize patient, provider and health system factors.
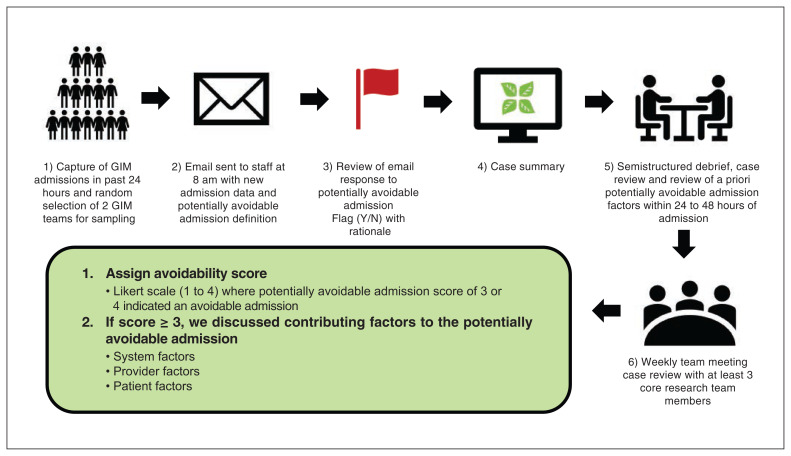
Methods: We conducted an observational study of GIM admissions at our institution from August 2019 to February 2020. We defined potentially avoidable admissions as admissions that could be managed in an appropriate and safe manner in the emergency department or ambulatory setting and asked staff physicians to screen admissions daily and flag candidates as potentially avoidable admissions. For each candidate, we prepared a case review and debriefed with members of the admitting team. We then reviewed each candidate with our research team, assigned an avoidability score (1 [low] to 4 [high]) and identified contributing factors for those with scores of 3 or more.
Results: We screened 601 total admissions and staff physicians flagged 117 (19.5%) of these as candidate potential avoidable admissions. Consensus review identified 67 candidates as potentially avoidable admissions (11.1%, 95% confidence interval 8.8%-13.9%); these patients were younger (mean age 65 yr v. 72 yr), had fewer comorbidities (Canadian Institute for Health Information Case Mix Group+ 0.42 v. 1.14), had lower resource-intensity weighting scores (0.72 v. 1.50) and shorter hospital lengths of stay (29 h v. 105 h) (p < 0.01). Common factors included diagnostic and therapeutic uncertainty, perceived need for short-term monitoring, government directive of a 4-hour limit for admission decision-making and subspecialist request to admit.
Interpretation: Our prospective method of screening, flagging and case review showed that 1 in 9 GIM admissions were potentially avoidable. Other institutions could consider adapting this methodology to ascertain their rate of potentially avoidable admissions and to understand contributing factors to inform improvement endeavours.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


