Jesse Elliott, Shannon E Kelly, Zemin Bai, Becky Skidmore, Michel Boucher, Derek So, George A Wells
{"title":"临床重要患者亚组经皮冠状动脉介入治疗后延长双重抗血小板治疗:系统回顾和荟萃分析。","authors":"Jesse Elliott, Shannon E Kelly, Zemin Bai, Becky Skidmore, Michel Boucher, Derek So, George A Wells","doi":"10.9778/cmajo.20210119","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Dual antiplatelet therapy (DAPT) is routinely given to patients after percutaneous coronary intervention (PCI) with stenting; however, optimal duration remains uncertain in some situations. We assessed the benefits and harms of extending DAPT beyond 1 year after PCI in clinically important patient subgroups.</p><p><strong>Methods: </strong>We conducted a systematic review and meta-analysis. We searched electronic databases (Embase, MEDLINE, PubMed, Cochrane Library) and grey literature (from inception to Nov. 5, 2021) and included randomized controlled trials (RCTs) of extended DAPT (> 12 mo) compared with DAPT for 6-12 months following PCI with stenting. The primary outcome was death (all cause, cardiovascular, noncardiovascular); secondary outcomes included major adverse cardiovascular and cerebrovascular events, myocardial infarction (MI), stroke, stent thrombosis and bleeding. Subgroups were based on prespecified patient characteristics (prior MI, acute coronary syndrome [ACS], diabetes mellitus, age, smoking status). Data were analyzed by random-effects pairwise meta-analysis.</p><p><strong>Results: </strong>We identified 9 RCTs that provided subgroup data. We found that extended DAPT reduced the risk of MI and stent thrombosis but increased the risk of bleeding, compared with standard DAPT, with no difference in the risk of all-cause death (relative risk [RR] 1.07, 95% confidence interval [CI] 0.80-1.42) or cardiovascular death (RR 0.98, 95% CI 0.74-1.30). We found that patients with a prior MI, with ACS at presentation, without diabetes or aged younger than 75 years may derive the most benefit from extended DAPT. Among patients who received extended DAPT, the risk of all-cause death was significantly increased among those with no prior MI (RR 1.64, 95% CI 1.08-2.24), whereas there was no significant difference in the risk of all-cause death between standard and extended DAPT for patients with ACS (RR 1.20, 95% CI 0.51-2.83), with diabetes (RR 1.27, 95% CI 0.86-1.89), aged older than 75 years (RR 1.32, 95% CI 0.39-4.54) or who smoked (RR 0.90, 95% CI 0.42-1.92). Similar results were found for cardiovascular death, where data were available.</p><p><strong>Interpretation: </strong>Patients with a previous MI with ACS at presentation, without diabetes, or aged younger than 75 years may derive the most benefit from extended DAPT. These findings support the need for careful selection of patients who may benefit most from extended DAPT.</p><p><strong>Study registration: </strong>PROSPERO no. CRD42018082587.</p>","PeriodicalId":10432,"journal":{"name":"CMAJ open","volume":"11 1","pages":"E118-E130"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f9/e1/cmajo.20210119.PMC9911127.pdf","citationCount":"1","resultStr":"{\"title\":\"Extended dual antiplatelet therapy following percutaneous coronary intervention in clinically important patient subgroups: a systematic review and meta-analysis.\",\"authors\":\"Jesse Elliott, Shannon E Kelly, Zemin Bai, Becky Skidmore, Michel Boucher, Derek So, George A Wells\",\"doi\":\"10.9778/cmajo.20210119\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Dual antiplatelet therapy (DAPT) is routinely given to patients after percutaneous coronary intervention (PCI) with stenting; however, optimal duration remains uncertain in some situations. We assessed the benefits and harms of extending DAPT beyond 1 year after PCI in clinically important patient subgroups.</p><p><strong>Methods: </strong>We conducted a systematic review and meta-analysis. We searched electronic databases (Embase, MEDLINE, PubMed, Cochrane Library) and grey literature (from inception to Nov. 5, 2021) and included randomized controlled trials (RCTs) of extended DAPT (> 12 mo) compared with DAPT for 6-12 months following PCI with stenting. The primary outcome was death (all cause, cardiovascular, noncardiovascular); secondary outcomes included major adverse cardiovascular and cerebrovascular events, myocardial infarction (MI), stroke, stent thrombosis and bleeding. Subgroups were based on prespecified patient characteristics (prior MI, acute coronary syndrome [ACS], diabetes mellitus, age, smoking status). Data were analyzed by random-effects pairwise meta-analysis.</p><p><strong>Results: </strong>We identified 9 RCTs that provided subgroup data. We found that extended DAPT reduced the risk of MI and stent thrombosis but increased the risk of bleeding, compared with standard DAPT, with no difference in the risk of all-cause death (relative risk [RR] 1.07, 95% confidence interval [CI] 0.80-1.42) or cardiovascular death (RR 0.98, 95% CI 0.74-1.30). We found that patients with a prior MI, with ACS at presentation, without diabetes or aged younger than 75 years may derive the most benefit from extended DAPT. Among patients who received extended DAPT, the risk of all-cause death was significantly increased among those with no prior MI (RR 1.64, 95% CI 1.08-2.24), whereas there was no significant difference in the risk of all-cause death between standard and extended DAPT for patients with ACS (RR 1.20, 95% CI 0.51-2.83), with diabetes (RR 1.27, 95% CI 0.86-1.89), aged older than 75 years (RR 1.32, 95% CI 0.39-4.54) or who smoked (RR 0.90, 95% CI 0.42-1.92). Similar results were found for cardiovascular death, where data were available.</p><p><strong>Interpretation: </strong>Patients with a previous MI with ACS at presentation, without diabetes, or aged younger than 75 years may derive the most benefit from extended DAPT. These findings support the need for careful selection of patients who may benefit most from extended DAPT.</p><p><strong>Study registration: </strong>PROSPERO no. CRD42018082587.</p>\",\"PeriodicalId\":10432,\"journal\":{\"name\":\"CMAJ open\",\"volume\":\"11 1\",\"pages\":\"E118-E130\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f9/e1/cmajo.20210119.PMC9911127.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"CMAJ open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.9778/cmajo.20210119\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"CMAJ open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.9778/cmajo.20210119","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
摘要
背景:双重抗血小板治疗(DAPT)常规给予经皮冠状动脉介入治疗(PCI)支架植入术后的患者;然而,在某些情况下,最佳持续时间仍然不确定。我们评估了临床上重要的患者亚组在PCI后延长DAPT超过1年的利与弊。方法:我们进行了系统综述和荟萃分析。我们检索了电子数据库(Embase, MEDLINE, PubMed, Cochrane Library)和灰色文献(从创建到2021年11月5日),并纳入了延长DAPT(> 12个月)与PCI支架置入后6-12个月DAPT的随机对照试验(rct)。主要结局是死亡(全因,心血管和非心血管);次要结局包括主要不良心脑血管事件、心肌梗死(MI)、中风、支架血栓形成和出血。亚组基于预先指定的患者特征(既往心肌梗死、急性冠脉综合征(ACS)、糖尿病、年龄、吸烟状况)。数据采用随机效应两两荟萃分析。结果:我们确定了9个提供亚组数据的随机对照试验。我们发现,与标准DAPT相比,延长DAPT降低了心肌梗死和支架血栓形成的风险,但增加了出血的风险,在全因死亡风险(相对风险[RR] 1.07, 95%可信区间[CI] 0.80-1.42)或心血管死亡风险(RR 0.98, 95% CI 0.74-1.30)方面没有差异。我们发现既往心肌梗死、首发时伴有ACS、无糖尿病或年龄小于75岁的患者可能从延长DAPT中获益最多。在接受延长DAPT治疗的患者中,无心肌梗塞患者的全因死亡风险显著增加(RR 1.64, 95% CI 1.08-2.24),而ACS患者(RR 1.20, 95% CI 0.51-2.83)、糖尿病患者(RR 1.27, 95% CI 0.86-1.89)、75岁以上患者(RR 1.32, 95% CI 0.39-4.54)或吸烟患者(RR 0.90, 95% CI 0.42-1.92)的标准DAPT治疗与延长DAPT治疗的全因死亡风险无显著差异。在可获得数据的心血管死亡中也发现了类似的结果。解释:既往心肌梗死合并ACS,无糖尿病或年龄小于75岁的患者可能从延长DAPT中获益最多。这些发现支持仔细选择可能从延长DAPT获益最多的患者的必要性。学习登记:普洛斯彼罗号。CRD42018082587。
Extended dual antiplatelet therapy following percutaneous coronary intervention in clinically important patient subgroups: a systematic review and meta-analysis.
Background: Dual antiplatelet therapy (DAPT) is routinely given to patients after percutaneous coronary intervention (PCI) with stenting; however, optimal duration remains uncertain in some situations. We assessed the benefits and harms of extending DAPT beyond 1 year after PCI in clinically important patient subgroups.
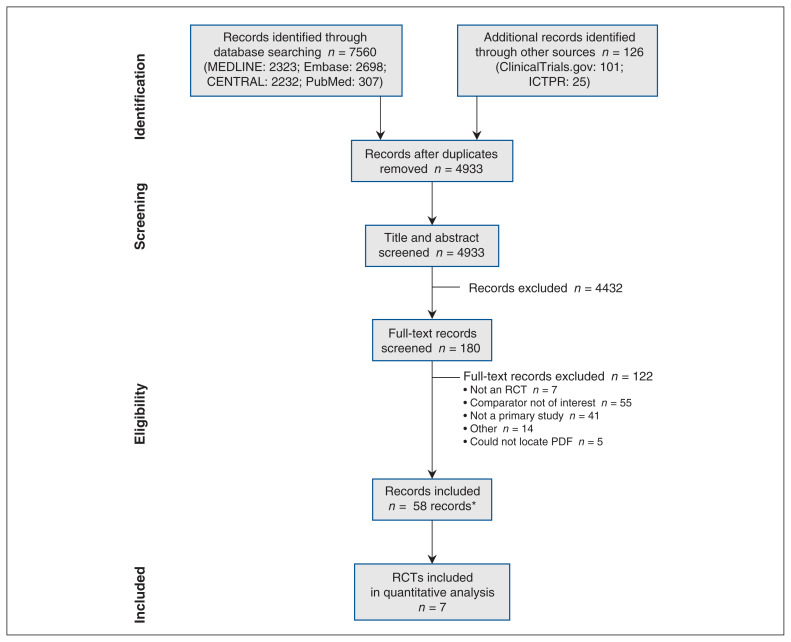
Methods: We conducted a systematic review and meta-analysis. We searched electronic databases (Embase, MEDLINE, PubMed, Cochrane Library) and grey literature (from inception to Nov. 5, 2021) and included randomized controlled trials (RCTs) of extended DAPT (> 12 mo) compared with DAPT for 6-12 months following PCI with stenting. The primary outcome was death (all cause, cardiovascular, noncardiovascular); secondary outcomes included major adverse cardiovascular and cerebrovascular events, myocardial infarction (MI), stroke, stent thrombosis and bleeding. Subgroups were based on prespecified patient characteristics (prior MI, acute coronary syndrome [ACS], diabetes mellitus, age, smoking status). Data were analyzed by random-effects pairwise meta-analysis.
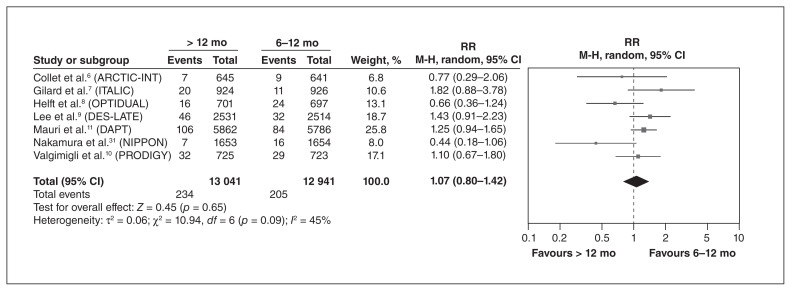
Results: We identified 9 RCTs that provided subgroup data. We found that extended DAPT reduced the risk of MI and stent thrombosis but increased the risk of bleeding, compared with standard DAPT, with no difference in the risk of all-cause death (relative risk [RR] 1.07, 95% confidence interval [CI] 0.80-1.42) or cardiovascular death (RR 0.98, 95% CI 0.74-1.30). We found that patients with a prior MI, with ACS at presentation, without diabetes or aged younger than 75 years may derive the most benefit from extended DAPT. Among patients who received extended DAPT, the risk of all-cause death was significantly increased among those with no prior MI (RR 1.64, 95% CI 1.08-2.24), whereas there was no significant difference in the risk of all-cause death between standard and extended DAPT for patients with ACS (RR 1.20, 95% CI 0.51-2.83), with diabetes (RR 1.27, 95% CI 0.86-1.89), aged older than 75 years (RR 1.32, 95% CI 0.39-4.54) or who smoked (RR 0.90, 95% CI 0.42-1.92). Similar results were found for cardiovascular death, where data were available.
Interpretation: Patients with a previous MI with ACS at presentation, without diabetes, or aged younger than 75 years may derive the most benefit from extended DAPT. These findings support the need for careful selection of patients who may benefit most from extended DAPT.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


