Adriana M Hung, Amber J Hackstadt, Marie R Griffin, Carlos G Grijalva, Robert A Greevy, Christianne L Roumie
{"title":"二甲双胍与磺脲类药物对肾功能减退患者肾功能下降或死亡的比较疗效:一项回顾性队列研究","authors":"Adriana M Hung, Amber J Hackstadt, Marie R Griffin, Carlos G Grijalva, Robert A Greevy, Christianne L Roumie","doi":"10.9778/cmajo.20210207","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Diabetes often causes kidney disease. In this study, we sought to evaluate if metformin use was associated with death or kidney events in patients with diabetes and concurrent reduced kidney function.</p><p><strong>Methods: </strong>We used data from the Veterans Health Administration, Medicare and National Death Index databases to assemble a national retrospective cohort of veterans who were using metformin or sulfonylureas from 2001 through 2016 and who began follow-up at an estimated glomerular filtration rate (eGFR) of less than 60 mL/min/1.73 m<sup>2</sup>. The primary composite outcome was a kidney event (i.e., 40% decline in eGFR or end-stage renal disease) or death. The secondary outcome was a kidney event (eGFR decline or end-stage renal disease). We weighted the cohort using propensity scores and used Cox proportional models to estimate the cause-specific hazard of outcomes and of treatment nonpersistence as a competing risk. We stratified follow-up into 2 periods, namely the first 360 days from the start of follow-up, and 361 days and beyond.</p><p><strong>Results: </strong>In the first 360 days, the propensity score-weighted cohort included 24 883 patients who used metformin and 24 998 who used sulfonylureas. There were 33.5 (95% confidence interval [CI] 30.9-36.3) and 43.0 (95% CI 40.1-46.0) deaths or kidney events per 1000 person-years for patients who used metformin or sulfonylureas, respectively (hazard ratio [HR] 0.78, 95% CI 0.71-0.85). For the secondary outcome of kidney events, the HR was 0.94 (95% CI 0.67-1.33). In the second period from 361 days onward, the primary outcome event rate was 26.5 (95% CI 24.7-28.5) per 1000 person-years for those who used metformin, compared with 36.3 (95% CI 34.2-38.6) per 1000 person-years for those who used sulfonylureas (HR 0.73, 95% CI 0.67-0.79). Results were consistent for kidney events alone (HR 0.73, 95% CI 0.59-0.91).</p><p><strong>Interpretation: </strong>Metformin use for 361 days or longer after reaching an eGFR of less than 60 mL/min/1.73 m<sup>2</sup> was associated with decreased likelihood of kidney events or death in patients with diabetes, compared with use of sulfonylureas. Metformin provided end-organ protection, in addition to glucose control.</p>","PeriodicalId":10432,"journal":{"name":"CMAJ open","volume":"11 1","pages":"E77-E89"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/39/04/cmajo.20210207.PMC9894655.pdf","citationCount":"1","resultStr":"{\"title\":\"Comparative effectiveness of metformin versus sulfonylureas on kidney function decline or death among patients with reduced kidney function: a retrospective cohort study.\",\"authors\":\"Adriana M Hung, Amber J Hackstadt, Marie R Griffin, Carlos G Grijalva, Robert A Greevy, Christianne L Roumie\",\"doi\":\"10.9778/cmajo.20210207\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Diabetes often causes kidney disease. In this study, we sought to evaluate if metformin use was associated with death or kidney events in patients with diabetes and concurrent reduced kidney function.</p><p><strong>Methods: </strong>We used data from the Veterans Health Administration, Medicare and National Death Index databases to assemble a national retrospective cohort of veterans who were using metformin or sulfonylureas from 2001 through 2016 and who began follow-up at an estimated glomerular filtration rate (eGFR) of less than 60 mL/min/1.73 m<sup>2</sup>. The primary composite outcome was a kidney event (i.e., 40% decline in eGFR or end-stage renal disease) or death. The secondary outcome was a kidney event (eGFR decline or end-stage renal disease). We weighted the cohort using propensity scores and used Cox proportional models to estimate the cause-specific hazard of outcomes and of treatment nonpersistence as a competing risk. We stratified follow-up into 2 periods, namely the first 360 days from the start of follow-up, and 361 days and beyond.</p><p><strong>Results: </strong>In the first 360 days, the propensity score-weighted cohort included 24 883 patients who used metformin and 24 998 who used sulfonylureas. There were 33.5 (95% confidence interval [CI] 30.9-36.3) and 43.0 (95% CI 40.1-46.0) deaths or kidney events per 1000 person-years for patients who used metformin or sulfonylureas, respectively (hazard ratio [HR] 0.78, 95% CI 0.71-0.85). For the secondary outcome of kidney events, the HR was 0.94 (95% CI 0.67-1.33). In the second period from 361 days onward, the primary outcome event rate was 26.5 (95% CI 24.7-28.5) per 1000 person-years for those who used metformin, compared with 36.3 (95% CI 34.2-38.6) per 1000 person-years for those who used sulfonylureas (HR 0.73, 95% CI 0.67-0.79). Results were consistent for kidney events alone (HR 0.73, 95% CI 0.59-0.91).</p><p><strong>Interpretation: </strong>Metformin use for 361 days or longer after reaching an eGFR of less than 60 mL/min/1.73 m<sup>2</sup> was associated with decreased likelihood of kidney events or death in patients with diabetes, compared with use of sulfonylureas. Metformin provided end-organ protection, in addition to glucose control.</p>\",\"PeriodicalId\":10432,\"journal\":{\"name\":\"CMAJ open\",\"volume\":\"11 1\",\"pages\":\"E77-E89\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/39/04/cmajo.20210207.PMC9894655.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"CMAJ open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.9778/cmajo.20210207\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"CMAJ open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.9778/cmajo.20210207","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
摘要
背景:糖尿病常引起肾脏疾病。在这项研究中,我们试图评估二甲双胍的使用是否与糖尿病患者的死亡或肾脏事件相关,并伴有肾功能下降。方法:我们使用来自退伍军人健康管理局、医疗保险和国家死亡指数数据库的数据,对2001年至2016年使用二甲双胍或磺脲类药物的退伍军人进行全国回顾性队列研究,这些退伍军人的肾小球滤过率(eGFR)估计小于60 mL/min/1.73 m2。主要综合结局是肾脏事件(即eGFR下降40%或终末期肾脏疾病)或死亡。次要结局是肾脏事件(eGFR下降或终末期肾脏疾病)。我们使用倾向评分对队列进行加权,并使用Cox比例模型来估计结果的病因特异性风险和治疗不持续性作为竞争风险。我们将随访分为2个阶段,即开始随访后的前360天和361天及以后。结果:在前360天,倾向评分加权队列包括24883例使用二甲双胍的患者和24998例使用磺脲类药物的患者。使用二甲双胍或磺脲类药物的患者每1000人年分别有33.5例(95%可信区间[CI] 30.9-36.3)和43.0例(95% CI 40.1-46.0)死亡或肾脏事件(风险比[HR] 0.78, 95% CI 0.71-0.85)。对于肾脏事件的次要结局,HR为0.94 (95% CI 0.67-1.33)。从361天开始的第二个阶段,使用二甲双胍的患者的主要结局事件发生率为每1000人年26.5例(95% CI 24.7-28.5),而使用磺脲类药物的患者的主要结局事件发生率为每1000人年36.3例(95% CI 34.2-38.6) (HR 0.73, 95% CI 0.67-0.79)。单独肾脏事件的结果是一致的(HR 0.73, 95% CI 0.59-0.91)。解释:与使用磺脲类药物相比,在eGFR低于60 mL/min/1.73 m2后,使用二甲双胍361天或更长时间与糖尿病患者肾脏事件或死亡的可能性降低相关。二甲双胍除了控制血糖外,还提供末端器官保护。
Comparative effectiveness of metformin versus sulfonylureas on kidney function decline or death among patients with reduced kidney function: a retrospective cohort study.
Background: Diabetes often causes kidney disease. In this study, we sought to evaluate if metformin use was associated with death or kidney events in patients with diabetes and concurrent reduced kidney function.
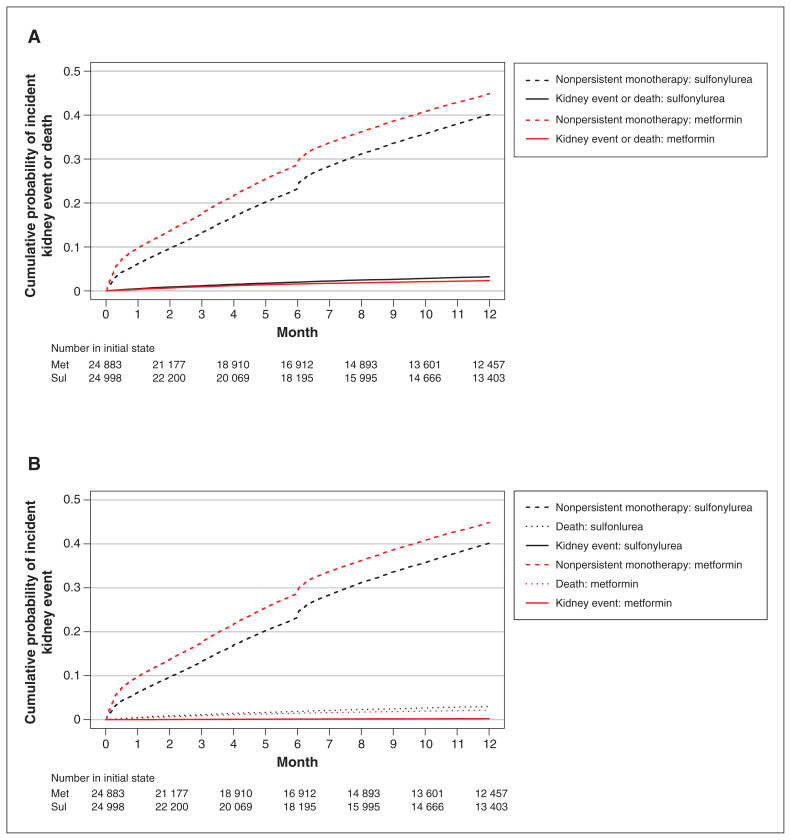
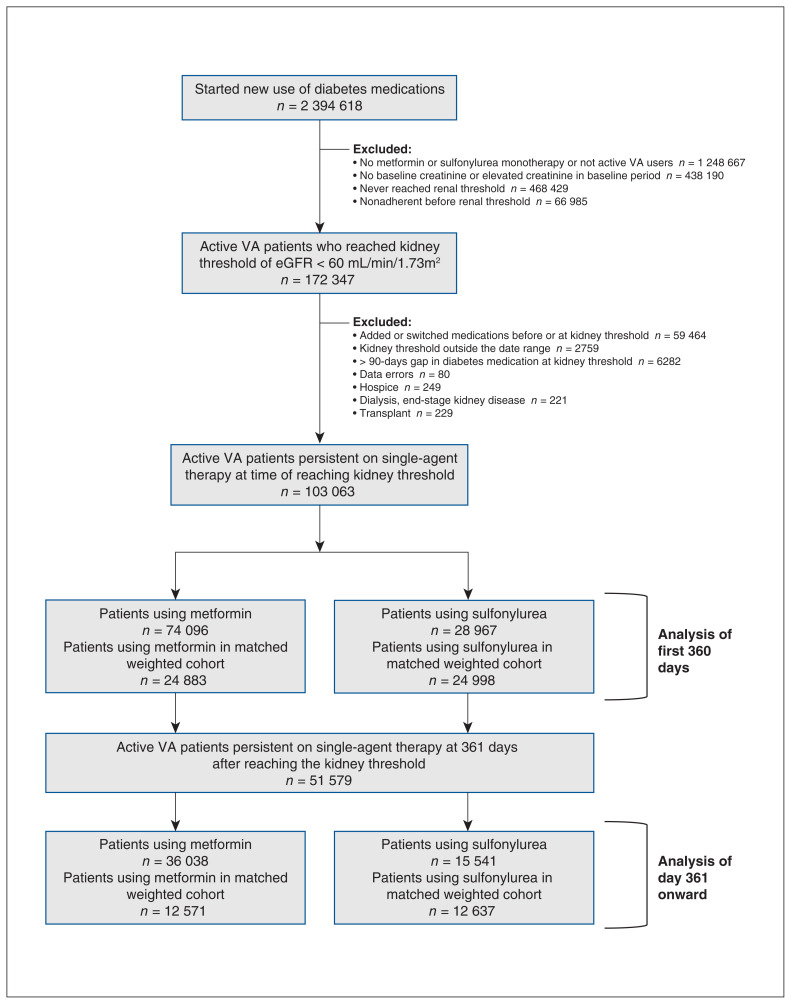
Methods: We used data from the Veterans Health Administration, Medicare and National Death Index databases to assemble a national retrospective cohort of veterans who were using metformin or sulfonylureas from 2001 through 2016 and who began follow-up at an estimated glomerular filtration rate (eGFR) of less than 60 mL/min/1.73 m2. The primary composite outcome was a kidney event (i.e., 40% decline in eGFR or end-stage renal disease) or death. The secondary outcome was a kidney event (eGFR decline or end-stage renal disease). We weighted the cohort using propensity scores and used Cox proportional models to estimate the cause-specific hazard of outcomes and of treatment nonpersistence as a competing risk. We stratified follow-up into 2 periods, namely the first 360 days from the start of follow-up, and 361 days and beyond.
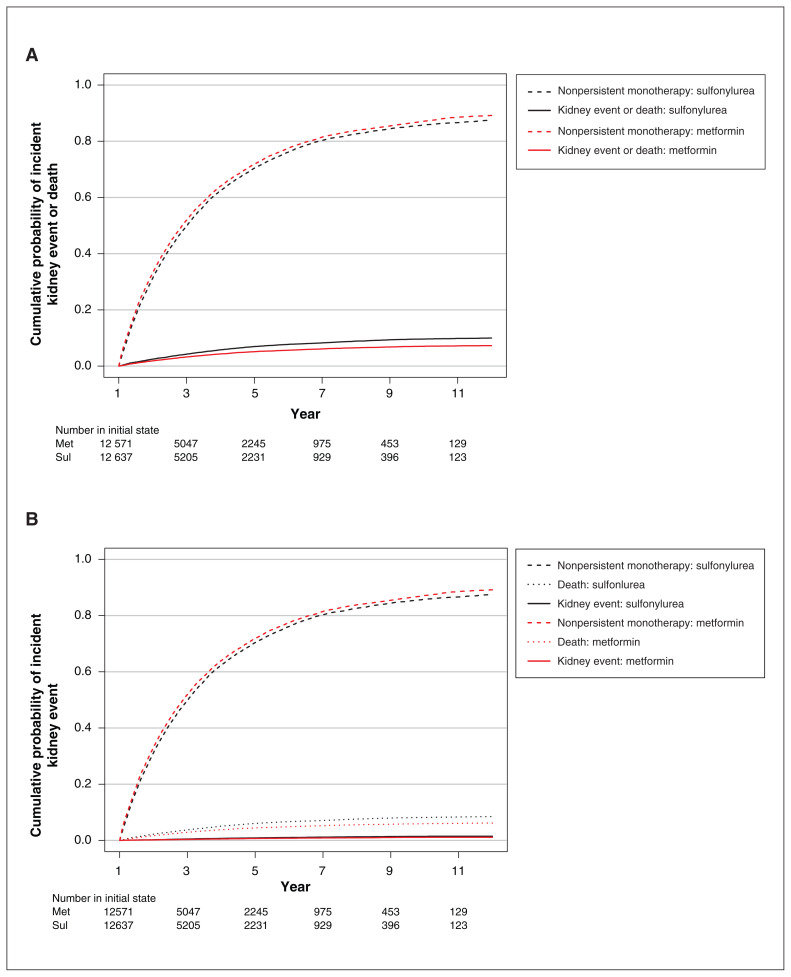
Results: In the first 360 days, the propensity score-weighted cohort included 24 883 patients who used metformin and 24 998 who used sulfonylureas. There were 33.5 (95% confidence interval [CI] 30.9-36.3) and 43.0 (95% CI 40.1-46.0) deaths or kidney events per 1000 person-years for patients who used metformin or sulfonylureas, respectively (hazard ratio [HR] 0.78, 95% CI 0.71-0.85). For the secondary outcome of kidney events, the HR was 0.94 (95% CI 0.67-1.33). In the second period from 361 days onward, the primary outcome event rate was 26.5 (95% CI 24.7-28.5) per 1000 person-years for those who used metformin, compared with 36.3 (95% CI 34.2-38.6) per 1000 person-years for those who used sulfonylureas (HR 0.73, 95% CI 0.67-0.79). Results were consistent for kidney events alone (HR 0.73, 95% CI 0.59-0.91).
Interpretation: Metformin use for 361 days or longer after reaching an eGFR of less than 60 mL/min/1.73 m2 was associated with decreased likelihood of kidney events or death in patients with diabetes, compared with use of sulfonylureas. Metformin provided end-organ protection, in addition to glucose control.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


