Husam H. Balkhy MD , Eugene A. Grossi MD , Bob Kiaii MD , Douglas Murphy MD , Arnar Geirsson MD , Sloane Guy MD , Clifton Lewis MD
{"title":"微创二尖瓣手术中主动脉内球囊闭塞与体外夹闭的回顾性评估比较","authors":"Husam H. Balkhy MD , Eugene A. Grossi MD , Bob Kiaii MD , Douglas Murphy MD , Arnar Geirsson MD , Sloane Guy MD , Clifton Lewis MD","doi":"10.1053/j.semtcvs.2022.11.016","DOIUrl":null,"url":null,"abstract":"<div><p><span><span><span><span><span>We compare outcomes of endo-aortic balloon occlusion (EABO) vs external </span>aortic clamping (EAC) </span>in patients<span> undergoing minimally invasive mitral valve surgery (MIMVS) in the Society of Thoracic Surgeons (STS) Adult Cardiac Surgery Database. Adults undergoing mitral valve surgery (July 2017–December 2018) were identified within the STS database (N = 60,607). Total 7,978 patients underwent a minimally invasive approach (including robotically assisted). About 1,163 EABO patients were 1:1 propensity-matched to EAC patients using exact matching on age, sex, and type of mitral procedure, and propensity score average matching for 16 other risk indicators. Early outcomes were compared. Categorical variables were compared using </span></span>logistic regression; hospital and </span>intensive care unit<span> length of stay were compared using negative binomial regression. In the matched cohort, mean age was 62 years; 35.9% were female, and 86% underwent mitral valve repair<span>. Cardiopulmonary bypass time was shorter for EABO vs EAC group (125.0 ± 53.0 vs 134.0 ± 67.0 minutes, </span></span></span><em>P</em><span> = 0.0009). There was one aortic dissection in the EAC group and none in the EABO group (</span><em>P</em><span> value > 0.31), and no statistically significant differences in cross-clamp time, major intraoperative bleeding, perioperative mortality, stroke, new onset of atrial fibrillation, postoperative acute kidney injury, success of repair. Median hospital LOS was shorter for EABO vs EAC procedures (4 vs 5 days, </span><em>P</em> < 0.0001). In this large, retrospective, STS database propensity-matched analysis ofpatients undergoing MIMVS, we observed similar safety outcomes for EABO and EAC, including no aortic dissections in the EABO group. The EABO group showed slightly shorter CPB times and hospital LOS.</p></div>","PeriodicalId":48592,"journal":{"name":"Seminars in Thoracic and Cardiovascular Surgery","volume":"36 1","pages":"Pages 27-36"},"PeriodicalIF":2.6000,"publicationDate":"2024-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"A Retrospective Evaluation of Endo-Aortic Balloon Occlusion Compared to External Clamping in Minimally Invasive Mitral Valve Surgery\",\"authors\":\"Husam H. Balkhy MD , Eugene A. Grossi MD , Bob Kiaii MD , Douglas Murphy MD , Arnar Geirsson MD , Sloane Guy MD , Clifton Lewis MD\",\"doi\":\"10.1053/j.semtcvs.2022.11.016\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><p><span><span><span><span><span>We compare outcomes of endo-aortic balloon occlusion (EABO) vs external </span>aortic clamping (EAC) </span>in patients<span> undergoing minimally invasive mitral valve surgery (MIMVS) in the Society of Thoracic Surgeons (STS) Adult Cardiac Surgery Database. Adults undergoing mitral valve surgery (July 2017–December 2018) were identified within the STS database (N = 60,607). Total 7,978 patients underwent a minimally invasive approach (including robotically assisted). About 1,163 EABO patients were 1:1 propensity-matched to EAC patients using exact matching on age, sex, and type of mitral procedure, and propensity score average matching for 16 other risk indicators. Early outcomes were compared. Categorical variables were compared using </span></span>logistic regression; hospital and </span>intensive care unit<span> length of stay were compared using negative binomial regression. In the matched cohort, mean age was 62 years; 35.9% were female, and 86% underwent mitral valve repair<span>. Cardiopulmonary bypass time was shorter for EABO vs EAC group (125.0 ± 53.0 vs 134.0 ± 67.0 minutes, </span></span></span><em>P</em><span> = 0.0009). There was one aortic dissection in the EAC group and none in the EABO group (</span><em>P</em><span> value > 0.31), and no statistically significant differences in cross-clamp time, major intraoperative bleeding, perioperative mortality, stroke, new onset of atrial fibrillation, postoperative acute kidney injury, success of repair. Median hospital LOS was shorter for EABO vs EAC procedures (4 vs 5 days, </span><em>P</em> < 0.0001). In this large, retrospective, STS database propensity-matched analysis ofpatients undergoing MIMVS, we observed similar safety outcomes for EABO and EAC, including no aortic dissections in the EABO group. The EABO group showed slightly shorter CPB times and hospital LOS.</p></div>\",\"PeriodicalId\":48592,\"journal\":{\"name\":\"Seminars in Thoracic and Cardiovascular Surgery\",\"volume\":\"36 1\",\"pages\":\"Pages 27-36\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2024-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Seminars in Thoracic and Cardiovascular Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S1043067923000400\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Seminars in Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1043067923000400","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
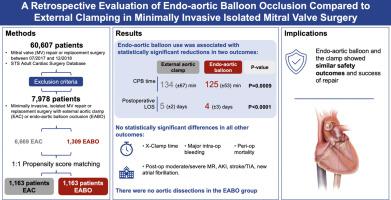
A Retrospective Evaluation of Endo-Aortic Balloon Occlusion Compared to External Clamping in Minimally Invasive Mitral Valve Surgery
We compare outcomes of endo-aortic balloon occlusion (EABO) vs external aortic clamping (EAC) in patients undergoing minimally invasive mitral valve surgery (MIMVS) in the Society of Thoracic Surgeons (STS) Adult Cardiac Surgery Database. Adults undergoing mitral valve surgery (July 2017–December 2018) were identified within the STS database (N = 60,607). Total 7,978 patients underwent a minimally invasive approach (including robotically assisted). About 1,163 EABO patients were 1:1 propensity-matched to EAC patients using exact matching on age, sex, and type of mitral procedure, and propensity score average matching for 16 other risk indicators. Early outcomes were compared. Categorical variables were compared using logistic regression; hospital and intensive care unit length of stay were compared using negative binomial regression. In the matched cohort, mean age was 62 years; 35.9% were female, and 86% underwent mitral valve repair. Cardiopulmonary bypass time was shorter for EABO vs EAC group (125.0 ± 53.0 vs 134.0 ± 67.0 minutes, P = 0.0009). There was one aortic dissection in the EAC group and none in the EABO group (P value > 0.31), and no statistically significant differences in cross-clamp time, major intraoperative bleeding, perioperative mortality, stroke, new onset of atrial fibrillation, postoperative acute kidney injury, success of repair. Median hospital LOS was shorter for EABO vs EAC procedures (4 vs 5 days, P < 0.0001). In this large, retrospective, STS database propensity-matched analysis ofpatients undergoing MIMVS, we observed similar safety outcomes for EABO and EAC, including no aortic dissections in the EABO group. The EABO group showed slightly shorter CPB times and hospital LOS.
期刊介绍:
Seminars in Thoracic and Cardiovascular Surgery is devoted to providing a forum for cardiothoracic surgeons to disseminate and discuss important new information and to gain insight into unresolved areas of question in the specialty. Each issue presents readers with a selection of original peer-reviewed articles accompanied by editorial commentary from specialists in the field. In addition, readers are offered valuable invited articles: State of Views editorials and Current Readings highlighting the latest contributions on central or controversial issues. Another prized feature is expert roundtable discussions in which experts debate critical questions for cardiothoracic treatment and care. Seminars is an invitation-only publication that receives original submissions transferred ONLY from its sister publication, The Journal of Thoracic and Cardiovascular Surgery. As we continue to expand the reach of the Journal, we will explore the possibility of accepting unsolicited manuscripts in the future.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


